Medicinal disease (LB) is a concept that combines a wide range of pathological effects of drugs, depending on or independent of the dose, that arise when they are used for therapeutic purposes. According to some authors, these conditions would be more correctly called adverse reactions of drugs (PRLS) or undesirable effects of drugs (NELS).
Etiology, pathogenesis, classification
I. Predictability:
| Types of reactions | Examples |
| 1. predictable (predictable) occur in 75% of cases. | |
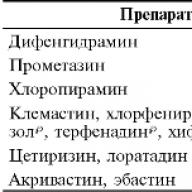
| · PRLS associated with the pharmacological properties of the drug | Sedation and drowsiness from use antihistamines |
| · Toxic complications resulting from an absolute or relative overdose | Ototoxic and nephrotoxic effects of aminoglycosides |
| · Secondary effects due to a violation of the immunobiological properties of the body | The development of dysbiosis and candidiasis with the use of powerful modern antibiotics |
| Cancellation syndrome | The occurrence of an exacerbation of the disease after the abolition of glucocorticosteroids |
| 2. Unpredictable occur in 25% of cases | |
| · Allergic (immunological) reactions of immediate and delayed types | PRLS associated with the development of hypersensitivity reactions of all types: anaphylactic shock, serum sickness, etc. |
| · Idiosyncrasy (an unusual reaction of the body to taking the drug) | Hemolytic anemia in the treatment of sulfonamides in patients with glucose-6-phosphate dehydrogenase deficiency. |
II. By severity:
The most common causes of death from PRLS and the drugs that can lead to these PRLS.
| PRLS | Preparations |
| GI bleeding and peptic ulcer | Corticosteroids, non-steroidal anti-inflammatory drugs (NSAIDs), anticoagulants |
| Bleeding (not from the digestive tract) | Anticoagulants, cytotoxic drugs |
| Aplastic anemia | Chloramphenicol, phenylbutazone, gold salts, cytotoxic drugs |
| Drug damage to the liver | Chlorpromazine, Isoniazid |
| Renal failure | Analgesics |
| Infectious complications | Corticosteroids, immunosuppressants |
| Anaphylactic reactions | Penicillins, antisera, etc. |
Clinical forms drug allergies
1. System PRLS
a. Anaphylactic shock (penicillin and other antibiotics)
b. Serum sickness (vaccines, serums)
c. Allergic vasculitis (allopurinol, myelosan, penicillins, phenothiazines, sulfonamides, tetracycline series)
2. Organ-specific syndromes (manifestations)
a. Hepatic Syndrome (halothane, aspirin, phenothiazines, azathioprine, erythromycin)
b. Renal Syndrome (methicillin, sulfonamides, cephalosporins)
c. Pulmonary Syndrome:
d. Skin reactions:
e. Gastrointestinal tract lesions in the form of allergic gastritis and enterocolitis
f. Hematological syndrome - anemia, granulocytopenia, thrombocytopenia.
Clinical picture and urgent events
The clinical symptoms of drug allergies are very diverse. They can be systemic, mainly skin, with selective damage to organs (lungs, liver, kidneys, etc.), hematological. Drug fever has been described as the only manifestation of drug allergy. Theoretically, all drugs can cause any syndrome, but observations show that certain syndromes are caused by certain drugs. In this work, only those that are of the greatest practical importance are listed as frequently occurring or difficult to proceed and life-threatening.
Anaphylactic shock
Anaphylactic shock is an acute, violent reaction mediated by Ig E. It develops in sensitized individuals to reintroduce a sensitizing agent.
Pathogenesis: antibody production → mast cell sensitization → circulating immune complexes (CICs) are formed upon repeated contact, mast cells are destroyed and a large number of biologically active substances (BAS) are released from them, which cause bronchospasm, pulmonary edema, vasodilation with the release of blood plasma tissue, a sharp drop in blood pressure, with prolonged development may appear arrhythmias and cardiogenic shock.
Clinic: 1-15 minutes after administration of the drug (sometimes immediately “on the needle”), the patient feels discomfort, anxiety, palpitations, paresthesias, itchy skin, throbbing in the ears, difficulty breathing. Signs of shock are: decreased blood pressure, involuntary urination and defecation, cramps, coma. Death may occur.
1. First-order events
a. Ensure airway, intubation is indicated in some cases
b. Adrenaline 0.3-0.5 ml solution in a dilution of 1: 1000 subcutaneously. If necessary, repeat again after 20 minutes. In especially severe cases, 0.5 under the tongue, intratracheally and / or intravenously, 1 mg in 250 ml of 5% glucose solution.
c. Replenishment of BCC - intravenous administration solutions of colloids and crystalloids in a total volume of up to 500-1000 ml;
d. With severe bronchospasm - inhalation of β-adrenergic agonists.
e. Corticosteroids: hydrocortisone 150-300 mg every 6 hours (prednisone 180 mg, dexamethasone 20 mg)
2. General events:
a. Aminophylline intravenously drip or stream slowly;
b. Puncture injection site with adrenaline
c. Activated charcoal 50-100 mg orally;
d. Antihistamines
e. Patients receiving β-blockers - glucagon 10 mg intravenously.
Observation of at least 6-24 hours with moderate reactions. In severe cases, hospitalization in the intensive care unit, ECG control is indicated.
Serum sickness
Serum sickness is an allergic reaction to heterologous serums or drugs, characterized by fever, arthralgia, skin rashes and lymphadenopathy. All these manifestations develop 3-5-12 days after the use of the drug. The frequency of development is 2-5%.
Etiology:
· Introduction of heterologous sera
· Introduction of heterologous immunoglobulins
· Introduction of tetanus toxoid
Skin symptoms (found in 85-95% of cases) - rashes, itching of the skin, urticaria.
Fever (70%)
Lymphadenopathy of all groups of lymph nodes
Joint lesions
Abdominal pain, nausea, vomiting, in severe cases with the development of gastrointestinal bleeding, melena (black stool) may appear.
Kidney damage
Neurological disorders in the form of peripheral nerve neuritis.
Myocarditis
By severity, mild, moderate, severe and extremely severe degrees are distinguished.
With a mild course and moderate severity, the use of antihistamines (diphenhydramine, pipolfen, suprastin, etc.) is sufficient.
In severe cases, glucocorticosteroids up to 0.5 mg / kg orally should be prescribed within 10-14 days.
For the prevention of serum sickness, it is necessary to carefully determine the allergic history. According to the anamnesis, two groups of individuals are distinguished: 1) persons who have never given allergic reactions (they are given “dangerous” drugs according to Unlimited - first 0.1 ml diluted 1:10 intradermally, after 30 minutes if there is no local or general intradermal reaction 0.1 ml is introduced in a 1: 1 dilution, if after 30 minutes there are no undesirable effects, then the remaining dose is administered intramuscularly); 2) Persons who have even experienced severe allergic reactions (such patients should be postponed, canceled, or administered under the guise of antihistamines and corticosteroids).
Urticaria and Quincke's edema
Almost all drugs that cause the development of anaphylactic shock and serum sickness can cause hives or angioedema. It is believed that these manifestations are rarely associated with the use of tetracyclines, allopurinol, digitalis preparations, anticoagulants when taken orally.
Medicinal rashes
The most common manifestations of PRLS are various skin lesions: itching, erythematous rash, maculopapular, scarlet-like and eczematous rashes [Zheltakov MM, Somov B.A., 1968]. Often in such cases, the term “medical dermatitis” is used, although in fact, there are no rashes that are characteristic only for drug-induced skin damage. Usually, rashes appear a few days after the start of the drug, often not on the 7-8th day, which is typical for allergic manifestations. As the causes of the rash, a lot of drugs are described. The mechanism for the development of rashes is unknown. There is an opinion that a cellular type of hypersensitivity plays a role in this, although accurate evidence of this has not yet been obtained. In most cases, the rash disappears within 3-4 days after drug withdrawal, but sometimes, despite drug withdrawal, it progresses to the degree of exfoliative dermatitis. Although in some cases skin rashes may be a manifestation of a underlying disease or a temporary change in reactivity (for example, penicillin rash with infectious mononucleosis), it is more correct to attribute “drug dermatitis” to allergic phenomena until another concept is proposed.
Fixed dermatitis
Limited areas of dermatitis with various single or multiple elements, sometimes large, from dark red spots to eczematous, vesicular or bullous, arising from repeated prescriptions of the “guilty” medication in the same places, are called fixed dermatitis. Localization can be any, including mucous membranes. General symptoms usually do not exist. A cellular type of hypersensitivity is suspected. More than 50 drugs are described as possible causes of fixed dermatitis.
Allergic vasculitis
Often severe, sometimes fatal reactions. In mild cases, only the skin is affected. Rashes usually appear on the lower extremities and can be erythematous, maculopapular and in the form of purpura. Sometimes part of the elements has the character of urtikarny. In some cases, purpura takes on a bullous and necrotic form. Systemic vasculitis is accompanied by fever, myalgia, arthritis, shortness of breath, headache, peripheral neuritis. Symptoms of bowel and kidney damage sometimes develop. During a histological examination, immunoglobulins and complement components are found in the walls of the vessels, which may indicate the immunocomplex nature of the process. In some cases, a decrease in the complement of blood serum is found, ESR is accelerated. Eosinophilia occurs intermittently, but with medicinal vasculitis more often than with other types. Presumably, some cases of nodular periarteritis are associated with drugs. Quite a lot of drugs have been described as etiological causes of vasculitis, among them are often used allopurinol, myelosan (busulfan), diphenhydramine, ethionamide, iodides, isoniazid, meprotan, diphenin, penicillins, phenythiazines, butadion, anaprilin (propranolol, obzidan) sulfonamides, tetracyclines, hypothiazide.
Drug fever
Medications can cause an increase in body temperature without allergies, for example, during the Yarish-Herksheimer reaction, contamination of fluids for parenteral use with exogenous pyrogens, release of endogenous pyrogens with aseptic inflammation. Stimulation of tissue metabolism (violation of oxidative phosphorylation during general anesthesia), peripheral vasoconstriction (the effect of norepinephrine) with a decrease in heat transfer and some other mechanisms are also possible. Fever naturally accompanies allergic immunocomplex reactions (serum-like, angiitis). IgE-dependent reactions are usually not accompanied by fever. Drug fever, as the only manifestation of an allergy, is extremely rare; its appearance is characteristic 7-14 days from the start of treatment with the drug. "Ninth day fever" is described in the treatment of syphilis with arsenic-containing drugs. With successful treatment of a febrile illness, the temperature usually drops for 3-5 days, and then rises again for 7-9 days of treatment. After discontinuation of the drug, the temperature normalizes in less than 48 hours. Repeated use of the same drug causes the rapid development of fever. The mechanism of this phenomenon is not exactly known. Many drugs, including antibacterials, are “guilty” of drug fever. Most often, it develops with the use of penicillins and cephalosporins, less often - sulfonamides, barbiturates, quinine. Drug fever is suppressed by corticosteroids.
Blood eosinophilia
Blood eosinophilia is rarely the only symptom of PRLS. Nevertheless, the growing eosinophilia during treatment with the drug serves as an occasion for its trial withdrawal and monitoring the further dynamics of this indicator. The relatively high frequency of eosinophilia in the treatment of kanamycin (about 10%) and prolonged streptomycin (about 50%). Often, eosinophilia is observed in the treatment of digitalis and its preparations, although the clinical manifestations of allergies are extremely rare.
Systemic lupus erythematosus (SLE) as a drug allergy syndrome.
The clinical syndrome, similar to the classic picture of SLE, is expressed by weakness, fever, damage to the serous membranes. Skin manifestations, lymphadenopathy, hepato- and splenomegaly are less permanent. In laboratory studies, increased ESR, leukopenia, LE cells and a positive reaction to antinuclear antibodies are found. The level of serum complement is normal, anti-DNA antibodies are not detected. In patients with hydralazine SLE, false positive RW occurs. The longer the treatment with the “guilty” drug, the more often antinuclear antibodies are detected. The genesis of the reaction remains unclear.
More or less documented cases of SLE are described with the use of apressin (hydralazine), procainamide, chlorpromazine, isoniazid (tubazide), penicillamine, diphenin (alepsin), praktolol. It is noted that for praktolol, a selective β 1 -adrenergic blocker, SLE is the most common adverse reaction. True drug SLE disappears within 1-2 weeks after discontinuation of the drug, although antinuclear antibodies can be detected for several months.
Medicinal allergic lesions of organs and systems.
Respiratory tract. Bronchospasm can be one of the manifestations of drug anaphylactic shock. Inhaled administration of a drug to a patient with previous anaphylactic sensitization to it can cause a bronchospastic reaction without concomitant manifestations. Allergic allergic asthma as a nosological form (and allergic rhinitis) develops with professional contact with medicines from pharmaceutical factory workers, pharmacists, and medical professionals. Perhaps the development of exogenous allergic alveolitis, eosinophilic infiltrates. In the first version, pituitrin and intal are described as causative factors, in the second - aminosalicylic acid, chlorpropamide (diabamide), intal, penicillin, sulfonamides, hypothiazide, methotrexate, nitrofurans. The latter, apparently, are the most common cause of acute pulmonary infiltrates, which develop in one of 400 treated.
Liver. It is suggested that the liver, which is directly involved in the metabolism of drugs, can often serve as a target organ for the development of drug allergies. Drug-induced liver damage is relatively common. They can be divided into two groups: 1) benign cholestatic hepatitis and 2) parenchymal hepatitis. In the first group, allergic genesis is most likely, because the disease usually begins with urticaria and arthralgia a few days after the start of treatment with the drug. Eosinophilia is determined in the blood. Then jaundice develops with all the signs of mechanical. After discontinuation of the drug, the condition normalizes within 2 weeks. Most often, drug cholestasis develops during treatment with chlorpromazine, in the second place is erythromycin; cases of liver damage with sulfanilamides, nitrofurans, nevigramone, etc. are described. Many people tend to consider parenchymal drug liver lesions as toxic rather than allergic.
The cardiovascular system. Medicinal allergic heart lesions are rarely isolated. Most often, focal myocarditis can be the result of serum-like reactions. Described eosinophilic myocarditis with a benign course of the type of eosinophilic Leffler infiltrate. The diagnosis is made on the basis of transient ECG changes combined with high eosinophilia.
Digestive organs. Symptoms of damage to the digestive apparatus, especially with the oral administration of drugs, are a very common manifestation of RLS. Some of them are regarded as allergic. So, allergic stomatitis, esophagitis, gastritis are described. Quincke's edema is often localized in the intestinal tissues, which is expressed by pain and symptoms of intestinal obstruction. In the small intestine, due to the peculiarities of its tissue structures (many mast cells), allergic reactions are localized especially often. Clinically, they are expressed by allergic diarrhea with profuse watery or mucous with an admixture of blood feces. Often these symptoms are combined with urticaria and eosinophilia.
Hematologic drug allergic syndromes.
Anemia, granulocytopenia, and thrombocytopenia are common manifestations of drug allergies.
There are suggestions that some syndromes, which until recently were considered a manifestation of drug allergies, are in fact due to bacterial, viral, mycoplasma infection and other factors. These syndromes include exfoliative dermatitis, toxic epidermal necrolysis (Lyell syndrome), Stevens-Johnson syndrome (erythema multiforme exudative with lesions of the skin and mucous membranes) and erythema nodosa.
Diagnostics
There is not a single method that would allow the doctor to reliably and without doubt diagnose drug allergies. This problem is complicated by the fact that in modern conditions the treatment of the disease requires the appointment of not one, but two or more drugs. In such cases, in the conditions of specialized allergological institutions, a comprehensive examination should be carried out, which allows with a certain degree of probability to confirm or reject an allergy to this drug.
The following factors are important for diagnosis:
- Anamnesis. Because for development allergic reaction the body should be sensitized to a specific drug, then there should be a history of taking this drug in the past. The presence of other types of atopy is also a factor contributing to the development of drug allergies. The cause of sensitization may be professional contact with drugs on the farm. enterprises, pharmacies, medical and veterinary institutions. Cross sensitization to various drugs is also possible.
- An allergic reaction does not depend on the dose of the drug (PRLS can develop as a result of using both the minimum and maximum doses)
- An allergic reaction usually fits into certain “classic” allergy syndromes.
- After the “guilty” drug is canceled, the reaction may disappear immediately, or it may last a few more days (which depends on the pharmacokinetic properties of individual drugs).
Skin tests if carried out incorrectly, they can lead to the development of anaphylactic shock and other life-threatening allergic reactions. Therefore, they should be carried out strictly according to the rules and according to indications. Indications for staging a skin-allergic test can be: 1) the inability to replace the drug with another, less effective, but safer; 2) if the patient has had prolonged professional contact with the medicine that is necessary for his treatment; 3) if the patient needs to prescribe a drug that previously gave allergic reactions in this patient; 4) if an allergic patient needs to be prescribed a highly allergenic drug, which he received earlier; 5) in case of vital indications for the appointment of penicillin to patients with fungal skin lesions (since a fungal skin lesion sensitizes the body to antibiotics of the penicillin group).
To identify an immediate type of reaction, scarification and intradermal tests are used. Dilution of drugs should be large (for example, penicillin is diluted from 0.5 to 100 U / ml). For most drugs, a negative skin reaction is not an indication of a complete absence of allergy to this drug. The exceptions are drugs related to full-fledged allergens (protein preparations, hormones, enzymes). When staging a skin test, in addition to the local reaction, a general reaction of the body may develop, sometimes of a severe degree. Therefore, a doctor who performs a cutaneous and especially an intradermal test should have an antishock kit ready in case of anaphylactic shock. To diagnose contact dermatitis, an application skin test is used. This test is quite informative and practically safe.
Provocative tests apply only in case of emergency in a specialized allergological hospital.
Laboratory methods . A huge number of laboratory tests proposed by different authors often do not provide reliable information about the presence or absence of allergies. Currently, the following tests are most often used: Shelley basophil degranulation, mast cell degranulation, histamine release by sensitized leukocytes, leukocyte blast transformation reaction (RBTL), leukocyte migration inhibition reaction (RTML). RAST is used to determine the antipenicillin IgE antibodies.
Prevention and treatment
Prevention of drug allergies can be divided into general and individual measures. General measures include, first and foremost, the fight against polypharmacy. This should also include the prohibition of the sale of drugs without prescription. Improving the production technology of non-synthetic hormones, replacing them with synthetic ones (for example, replacing ACTH with synactene) will definitely reduce the possibility of sensitization with foreign proteins. It is undesirable to use drugs as preservatives: acetylsalicylic acid when preserving fruits, chloramphenicol in the preparation of blood and plasma, penicillin for preserving meat during long-distance transport in hot weather.
Individual preventive measures include, first of all, careful attention to the patient's history. Many of the cases of lethal drug anaphylactic shock described in the literature are related to the fact that the patient was simply not asked whether he had been treated with this drug before and how he tolerated it.
To administer drugs to patients with a history of severe manifestations of drug allergy, separate syringes and needles must be used. Careful monitoring of the patient during the treatment period can help prevent a detailed reaction if "prodromal" symptoms are noted - itching, hyperemia of the skin at the injection site, manifestations of rhinitis and conjunctivitis (with inhalation), and increasing eosinophilia. The “prophylactic” administration of antihistamines does not prevent the development of allergic reactions to drugs.
A difficult situation arises when it is necessary to re-study using iodine-containing radiopaque substances in patients who underwent a reaction to a previous study. As indicated above, reactions to these drugs are currently regarded as pseudo-allergic, associated with histamine-blocking properties of the drug. Therefore, skin testing does not make sense. The introduction of a trial low dose is not currently applicable, because a reaction can develop not only at a high dose. Interestingly, the frequency of repeated reactions is not so great - 16-20%. If the second study has a vital indication, patients with a history of reaction are advised to pre-administer large doses of corticosteroids, for example, 40 mg of prednisone 3 times - every 6 hours before administration of contrast and 2 times after administration, as well as antihistamines.
Usually it is enough to discontinue the drug, which caused a mild allergic reaction of any genesis, so that the reaction underwent rapid reverse development. Severe acute and protracted reactions require treatment. Fundamentally, treatment does not differ from that for the corresponding syndromes of a different origin. In the acute period of severe reactions to the penicillin group of drugs, the introduction of 1,000,000 units of penicillinase, an enzyme of bacterial origin that destroys penicillins, is recommended in v / m. It should be remembered that methicillin, oxacillin and dicloxacillin are insensitive to penicillinase. If the reaction is caused by a phenothiazine-type drug - chlorpromazine, levomepromazine (tizercin), proprazine, frenolone, triftazine, thioridazine (meleryl), etc., diprazine (pipolfen), which also refers to phenothiazine derivatives, cannot be used as an atnistamine. With severe lesions of the skin, individual organs, blood system, vasculitis, corticosteroids are used (which in most cases gives a very good effect).
Epidemiology and etiology
Age Any.
Negative reactions to anticonvulsants are more common among blacks.
Etiology
Most often, anticonvulsants (phenytoin, carbamazepine, phenobarbital) and preparations containing a sulfonamide group. Less commonly, allopurinol, gold preparations, dapsone, sorbinil.
2-6 weeks after the start of treatment, later most of the other drug toxicides.
Prodromal period
Fever, rash.
General state
Fever.
Physical research
Key physiological indicators
Possible increase in body temperature.
Elements of a rash. First, a maculopapular rash (Fig. 22-4). In the future, exfoliative erythroderma may develop, especially if the drug is not canceled. As the rash resolves, peeling or detaching the epidermis. Color. Bright red. As the rash resolves, it is a brownish or purple hue.
Location Randomly arranged spots and papules that gradually merge. The rash is symmetrical. Localization. Almost always - the trunk and limbs. Sometimes a generalized rash occurs.
Mucous
There are rashes on the oral mucosa.
Other organs
Lymph nodes. Usually enlarged due to hyperplasia of lymphoid tissue. Internal organs. Damage to the heart, lungs, thyroid gland, liver, brain.
Differential diagnosis
Early stages
Viral infections (measles, rubella); drug rash; other diseases accompanied by measles rash. Late stages
Serum sickness, drug vasculitis, hemorrhagic vasculitis, cryoglobulinemia, infectious vasculitis, collagenoses.
Rash plus enlarged lymph nodes Rubella, cytomegalovirus infection (primary infection), infectious mononucleosis (primary infection).
Additional research
General blood analysis
Eosinophilia (in 30% of patients), atypical mononuclear cells.
Blood chemistry
Hepatitis-specific changes in biochemical parameters of liver function.
Pathomorphology
Leather. Perivascular lymphocytic and eosinophilic infiltration. Lymph nodes. Benign hyperplasia of lymphoid tissue. In rare cases, proliferation of atypical lymphocytes. The kidneys. Interstitial nephritis.
The clinical picture and histological examination of the affected organs.
Pathogenesis
Genetically determined slow oxidation (aromatic hydroxylation) of anticonvulsants; slow acetylation of preparations containing a sulfonamide group; hypersensitivity of leukocytes to hydroxylamine metabolites of dapsone.
Figure 22-4.
Symmetrical bright red rash, the elements of which merge in places. In addition, the patient has enlarged lymph nodes
The course and forecast
A side effect of anticonvulsants is manifested by facial swelling, exfoliative erythroderma, the appearance of blisters or hemorrhagic rash, fever, enlarged lymph nodes, eosinophilia, arthritis and hepatitis, which develops 2 weeks after the start of treatment and significantly worsens the prognosis. Deaths are rarely observed, for example due to eosinophilic myocarditis.
After drug withdrawal, rash and hepatitis may persist for several more weeks. In patients receiving corticosteroids, relapse is possible as their dose decreases. Hyperplasia of lymphoid tissue usually disappears after discontinuation of the drug, however, in rare cases, the development of lymphoma is possible.
Treatment and prevention
Identify the drug that caused the drug disease, and cancel it.
Symptomatic treatment
To quench the itching, N-blockers are prescribed inward.
Corticosteroids
Outdoor application. Maximum strength corticosteroids reduce itching, but usually do not affect the general condition of the patient. They are used 2 times a day. Ingestion. Prednisone at a dose of 0.5 mg / kg / day and above quickly leads to improvement and restoration of laboratory parameters.
Subsequent drug treatment
Due to hypersensitivity to other anticonvulsants containing an aromatic group, one should carefully select a drug for further treatment.
Prevention
The patient needs to be told that he has an increased sensitivity to a certain drug and, possibly, to other drugs of the same group. The drug that caused the drug disease cannot be re-prescribed. The patient is recommended to always have a list of contraindicated drugs (a card in his wallet or an identification bracelet).
Any clinical manifestations of the undesirable effects of drugs, especially requiring the use of special treatment methods, are considered a drug disease in the broad sense. Currently, most of the population of developed countries for various reasons constantly or periodically takes a variety of drugs. Modern pharmacotherapy has several features.
Highly selective, prolonged drugs have been developed.
There is a need for a long, often lifelong intake of drugs (antihypertensive, lipid-lowering drugs, antiplatelet agents, immunosuppressants).
Often, a large number of drugs are prescribed simultaneously (polypharmacy).
Uncontrolled intake of over-the-counter drugs (analgesics, sedatives and hypnotics) is possible.
Chapter 76. UNWANTED PHENOMENA (ADVERSE EFFECTS) OF MEDICINES
The prevalence of various undesirable effects in patients using drugs reaches 50%. The risk of developing unwanted effects is significantly higher in certain risk groups (Table 76-1). In addition to age, the likelihood of undesirable effects is affected by the failure of organs involved in the metabolism and excretion of drugs (primarily renal and hepatic). The dose and duration of taking the drugs are important, especially since some of them are able to accumulate in the body.
Table 76-1.Risk groups for adverse effects
According to the development mechanisms, undesirable effects can be divided into the following types.
Undesirable effects of drugs, which may be associated with the main effect of the drug. An example is the development of arterial hypotension when taking antihypertensive drugs (especially short-acting drugs), severe bradycardia and intracardiac conduction disturbances caused by p-adrenergic blockers and non-dihydropyridine blockers of slow calcium channels. Such undesirable effects depend on the dose of drugs, and they are usually described in the preclinical phase of trials of drugs and / or in studies on healthy volunteers.
Separately, it is worth considering undesirable effects caused by individual intolerance to drugs. Their clinical manifestations are non-specific and can often resemble systemic diseases.
Assessing the risk of their development is extremely difficult. Hypersensitivity to the drug - idiosyncrasy - is often genetically determined. More often it is based on congenital insufficiency of enzymes of the metabolism of drugs. Acquired idiosyncrasy is a consequence of past and / or chronic diseases.
A special place among the undesirable effects of drugs is occupied by allergic reactions. Their development does not depend on the dose of the drug. Serious
acute allergic reactions, such as:
Generalized bronchospasm;
Massive hemolysis;
Anaphylactic shock.
One of the most common allergy options is a variety of skin reactions in the form of a papular rash, urticaria, acne-like rashes.
Of great importance in establishing the undesirable effects of drugs belongs to clinical trials conducted in accordance with the rules. GCP (Good Clinical Practice- good clinical practice). Undesirable effects of drugs can be most reliably identified when comparing the effects of the drug and placebo. However, in many areas of clinical medicine, the use of a true placebo (i.e. dosage form, in appearance and organoleptic properties identical to the drug, but not containing the active substance) is unacceptable. In such cases, for comparison with the studied drugs use a drug with pre-established efficacy, safety and profile of undesirable effects. Assessment of unwanted effects is carried out on the basis of the severity of their course (table. 76-2).
Table 76-2.Classification of adverse effects by severity
Prospective studies reveal a special group of undesirable effects arising from prolonged use the drug, including those due to the cumulation of the drug itself or its toxic metabolites. In addition, with prolonged monitoring of patients taking drugs, it can be established its negative impact on the long-term prognosis, while with
short-term use of the drug is effective in stopping the symptoms of the disease, especially in the acute phase.
Of particular risk from the point of view of developing undesirable effects are drugs with the so-called narrow therapeutic range. These include:
Anticoagulants and some disaggregants;
Antiarrhythmic drugs;
Anticonvulsant and antipsychotic drugs;
Cardiac glycosides;
Methylxanthines;
Lithium preparations.
These drugs have a small range of doses that have a therapeutic effect, and even a slight excess can lead to drug intoxication.
Chapter 17 DRUG DISEASE
The term “drug disease” means nonspecific syndromes that have a similar clinical picture with systemic diseases and develop when drugs are prescribed, in the formation of which immunopathological reactions are involved. A drug disease can develop under the influence of any drug and is somewhat more common in women.
ETIOLOGY
The drugs that most often cause the development of a drug disease include:
Various antibacterial drugs;
NSAIDs;
Contrast substances used in conducting radiation research methods;
Vitamins (especially Group B).
Most drugs that cause drug illness, patients take on their own, without a doctor’s prescription. A clear relationship between the manifestations of a drug disease and the dose of the drug has not been established, but it is known that the likelihood of its development increases significantly with the simultaneous (often unreasonable) use of several drugs.
CLINICAL PICTURE
The clinical picture of drug disease is non-specific and is manifested by general symptoms of the disease and signs of damage to individual organs.
An increase in body temperature is one of the most frequent manifestations of a drug disease. Subfebrile condition that persists throughout the entire period of taking the drug is typical, but pronounced rises in body temperature (up to 39-40 ° C), accompanied by chills, are often observed. Fever more often occurs 1-2 weeks after
initiation of therapy, although it may appear immediately after the 1st dose of the drug.
The skin symptoms of a drug disease are diverse, many of them allergic in nature. One of the most characteristic variants of skin lesions is erythema nodosum, which is also observed with sarcoidosis, tuberculosis and malignant tumors.
Many drug-sick patients complain of joint pain (arthralgia). The options for articular syndrome in drug disease are diverse: from arthralgia, not accompanied by deformities, to typical arthritis, such as gouty when taking large doses of diuretics.
Hematological disorders are one of the most common manifestations of a drug disease (Table 77-1).
Agranulocytosis and hypoplastic anemia are considered the most prognostically unfavorable. Hypoplastic anemia is caused by chloramphenicol, many cytostatics. The last group of drugs, along with sulfonamides and antithyroid drugs, can also cause agranulocytosis.
Thrombocytopenia can develop during treatment with quinidine, gold preparations, sulfonamides, thiazide diuretics, as well as heparin, especially unfractionated.
Eosinophilia is one of the most common manifestations of a drug disease. With a significant increase in the content of eosinophils in the blood (\u003e 1.5 × 10 9 / L), various organs (lungs, heart) form infiltrates from these cells.
Many drugs can cause endocrine gland dysfunction. Most drug-induced endocrine gland dysfunctions are reversible and disappear when the dose is canceled or reduced.
The development of hyperprolactinemia can contribute to phenothiazines, haloperidol, monoamine oxidase inhibitors, tricyclic antidepressants, reserpine, methyldopa, metoclopramide, cocaine, verapamil, fluoxetine.
Preparations of some groups can affect the thyroid gland. In this case, hypothyroidism often develops (protionamide, ethionamide, lithium preparations, sulfonamides, interferons, amiodarone).
When taking HA, the Itsenko-Cushing drug syndrome is often formed.
Table 77-1.Hematologic manifestations of drug disease
The clinical picture of a drug disease can be similar to a systemic disease, more often with manifestations of periarteritis nodosa and SLE. The course of “systemic masks” of a drug disease is somewhat different from the corresponding diseases, for example, with drug SLE, kidney damage develops less often. However, in general, the course of systemic diseases induced by drugs can be very unfavorable.
Medicinal SLE can be caused by 5-aminosalicylic acid, chloroquine, hydralazine, isoniazid, phenylbutazone, tetracyclines, thiazide diuretics and some vaccines. The list of drugs that can induce these diseases is constantly updated by representatives of newly emerging classes of drugs, for example, streptokinase and some p-blockers.
Drug disease can take the form of any systemic vasculitis. A striking example of such lesions is the “epidemic” of periarteritis nodosa observed in Europe and the USA in the 1950s. and associated with the distribution of sulfonamides. Some drugs (allopurinol, isoniazid, phenothiazines) can cause necrotizing vasculitis associated with antibodies to neutrophil cytoplasm components. Special options for drug illness, debuting from skin lesions and posing a serious threat to the patient's life, include Stevens-Johnson and Lyell syndromes.
Stevens-Johnson syndrome is characterized by the appearance on the skin, mucous membranes of the mouth, upper respiratory tract and urethra and the conjunctiva of erythematous spots and blisters with hemorrhagic fluid. Patients have a pronounced intoxication syndrome (fever, arthralgia), often a widespread soft tissue necrosis develops.
With Lyell's syndrome (toxic epidermal necrolysis), widespread erythema suddenly appears, and later necrosis of the surface layers of the skin develops. As with Stevens-Johnson syndrome, marked signs of intoxication are noted. This variant of the drug disease can also lead to death. The clinical picture of drug disease often consists of predominantly single organ lesions.
In such cases, it is important to early recognize and eliminate the cause of the disease, as this often contributes to the reverse development of disorders.
Medicinal lung lesions
Forms of drug damage to the lungs
The most common non-specific pulmonary drug reactions include generalized bronchial obstruction, which develops, as a rule, acutely upon first contact with drugs and can lead to death from respiratory failure. Bronchial obstruction as a manifestation of individual hypersensitivity to the drug is often combined with Quincke's edema. The development of drug-induced bronchial asthma is associated primarily with the administration of acetylsalicylic acid and other NSAIDs.
- “Aspirin” asthma was described in the first 15 years from the date of receipt of acetylsalicylic acid. It has been established that the leading mediators of bronchial obstruction in "aspirin" asthma are leukotrienes formed from arachidonic acid under the action of lipoxygenase, which is activated during blockade of cyclooxygenase drugs. The disease is characterized by the dependence of attacks of bronchial obstruction on taking the appropriate drugs.
It is believed that there is a hereditary predisposition to "aspirin" asthma. When examining patients often
are the so-called aspirin triad, which includes the following components: ◊ polyposis of the upper respiratory tract; ◊ intolerance to aspirin ♠; ◊ bronchial asthma.
Management of a patient with “aspirin” asthma involves, first of all, elimination of contact with drugs that provoke an attack. To control bronchial obstruction, it is recommended to use leukotriene antagonists (zafirlukast) and inhaled HA.
Drugs can induce interstitial lung disease.
Acute and chronic forms of interstitial pulmonary disease induced by drugs are distinguished.
◊ Acute drug damage to the interstitium of the lungs, manifested mainly by fever and unproductive cough, can be regarded as pneumonia. Gradually, signs of respiratory failure join in - shortness of breath (often inspiratory), cyanosis and tachycardia. Eosinophilia is found in the blood. When chest x-rays reveal bilateral infiltrates, often localized in the basal and middle parts of the lungs. Spirography results indicate primarily a restrictive type of lung lesion. With CT in the lung tissue, it is possible to identify foci of active alveolitis (a symptom of "frosted glass").
◊ A chronic form of drug damage to pulmonary interstitium is characterized by an unproductive cough and slowly increasing shortness of breath. Fever and eosinophilia are observed much less frequently than in the acute variant. With prolonged use of the drug, diffuse fibrosis of pulmonary interstitium may develop.
Many antibacterial drugs (cephalosporins, sulfanilamides, penicillins, isoniazid) can cause damage to the interstitium of the lungs. The clinical picture of nitrofuran lung damage is similar to idiopathic fibrosing alveolitis. As a rule, drug withdrawal contributes to the remission of the disease, but in some cases it continues to progress. The absence of clinical improvement 2 months after the withdrawal of nitrofuran is an indication for the beginning of therapy with HA.
Diffuse fibrosis of pulmonary interstitium may develop in patients who receive amiodarone for a long time.
◊ It has been shown that the risk of developing an “amiodarone lung” is higher in patients receiving the drug at a dose of more than 400 mg / day or suffering from any chronic lung disease.
◊ The gradually increasing pulmonary interstitial fibrosis is considered the most common clinical variant of the “amiodarone lung”. In this case, increasing inspiratory dyspnea, unproductive cough, fever and weight loss are observed. In 10-20% of patients, pleural pain occurs. The x-ray picture does not differ from other variants of drug damage to pulmonary interstitium.
◊ In a number of cases, the clinical picture of the “amiodarone lung” is characterized by fever, and with an X-ray examination, localized infiltrates are detected in the lungs. This form of "amiodarone lung" is more often observed after surgical procedures performed under general anesthesia and angiographic procedures.
◊ The main treatment for all forms of “amiodarone lung” is the timely withdrawal of the drug. In cases where replacement of amiodarone with another antiarrhythmic drug is not possible, GC is prescribed.
Damage to pulmonary interstitium can develop with cytostatic therapy (methotrexate, cyclophosphamide, melphalan, chlorambucil, bleomycin). In patients receiving bleomycin, the frequency of this undesirable effect reaches 10%. The prognosis of bleomycin lung lesion is unfavorable: mortality reaches 50%. Factors that worsen the prognosis are old age, radiation therapy, oxygen treatment, a combination with other cytostatics, and a total dose of bleomycin in excess of 450 mg. For bleomycin lesions of the lungs, progression after the withdrawal of drugs and the low effectiveness of HA therapy are characteristic.
Many groups of drugs can also cause interstitial lung disease:
◊ anti-inflammatory drugs (gold preparations,
NSAIDs, phenylbutazone); ◊ anticonvulsant and antipsychotic drugs (phenyl
toin, carbamazepine, chlorpromazine);
◊ antiarrhythmic drugs [r-blockers (prop-
nolol, pindolol), procainamide]; ◊ antihypertensive drugs (hydralazine, hydrochlorothiazide).
Some drugs can cause acute respiratory distress syndrome. It is especially often observed in people who use drugs in inhaled forms (heroin, cocaine).
A peculiar variant of drug damage to the lungs was described in the 1960s, when drugs that reduce appetite, used to correct body weight, were widely used. When taking some representatives of this group of drugs, the development of damage to the vascular bed and lung interstitium was observed, indistinguishable from primary pulmonary hypertension. The disease continued to progress after drug withdrawal. In this regard, the appointment of the majority of representatives of this group of drugs was prohibited.
Medicinal lesions of the cardiovascular system
Many drugs used to treat cardiovascular diseases, when prescribed in inadequate doses, can cause the development of a variety of undesirable effects, which are usually an overly pronounced manifestation of their therapeutic effect. Excessive antihypertensive drugs cause arterial hypotension, and most antiarrhythmic drugs can have a proarrhythmic effect. However, undesirable effects from the cardiovascular system are also characteristic of drugs not used in cardiology practice (Table 77-2).
Table 77-2.Medications that cause damage to the cardiovascular system
In addition to the above violations, drugs can cause the following undesirable effects.
One of the most common adverse effects of drugs used to treat cardiovascular diseases is considered to be an extended interval syndrome. Q-T,diagnosed with increasing interval Q-Tmore than 440 ms.
Its clinical signs may include the development of fainting under stress and / or physical exertion and a tendency to bradycardia.
Family forms of the extended interval syndrome are distinguished. Q-T,for which, in addition to actually specific changes on the ECG, the presence of arrhythmias, sudden death, fainting (Romano-Ward syndrome) and deafness (Jerwell and Lange-Nielsen syndrome) in a family history is characteristic. Several genetic markers of extended interval syndrome have been identified Q-T,most of them encode individual forms of potassium and sodium channels.
Interval extension Q-Toften cause various medications:
◊ antiarrhythmic drugs classes:
♦ Ia - quinidine, procainamide, disopyramides;
♦ III - sotalol, amiodarone, ibutilide;
♦ IV - verapamil;
◊ psychotropic drugs (phenothiazines, haloperidol, tricyclic antidepressants, chloral hydrate);
The value of elongated syndrome Q-Tdetermined by the risk of complications - a variety of arrhythmias, including ventricular. Perhaps the development of ventricular tachycardia such as "pirouette" and sudden death. It should be borne in mind that only antiarrhythmic drugs of class Ia and III can directly cause an extension of the interval Q-T,due to the features of their mechanisms of action. The development of an extended interval syndrome Q-Twhen using other drugs, they are considered as idiosyncrasy. When an extended interval appears Q-T,as a rule, temporary withdrawal or reduction of the dose of drugs is required.
When appointing representatives of many classes of drugs, the development of myocarditis is described, however, verification of the diagnosis and assessment of the risk of this drug damage to the heart is very difficult. Cardiomyopathy induced by some cytostatics (doxorubicin, cyclophosphamide) is considered a more specific lesion of the cardiovascular system. Among the mechanisms of cardiotoxic action of these drugs, stimulation of the formation of free radicals and the release of catecholamines and histamine, which have a fibrogenic effect on the endocardium and myocardium, as well as inhibition of the synthesis of nucleic acids by cardiomyocytes, are distinguished.
The results of some epidemiological studies indicate that in patients receiving certain drugs (cyclosporine, antiretroviral drugs), acceleration of the progression of atherosclerosis is observed. However, in general, the role of drugs in the development of atherosclerosis remains unproven and still requires confirmation in studies.
Gastrointestinal tract
The most common manifestations of gastrointestinal drug damage are nausea, vomiting, and diarrhea.
Nausea and vomiting are the leading factors that worsen the tolerance of many cytostatic drugs.
Diarrhea can occur when prescribing various drugs:
Any laxative drugs in large doses;
Diuretics (furosemide, hydrochlorothiazide);
Methylxanthines;
Cholinergic drugs;
Cholinesterase inhibitors;
Quinidine;
Colchicine;
ACE inhibitors;
Blockers of H 2 receptors (ranitidine);
Antidepressants (selective serotonin reuptake inhibitors);
Prostaglandins (misoprostol).
One of the most common causes of drug-induced diarrhea in a population is antibacterial drugs. Among the intestinal complications of antibiotic therapy, pseudomembranous enterocolitis is of great importance. Pseudomembranous colitis is caused Clostridium difficile- a bacterium that multiplies in the colon when taking antibacterial drugs (cephalosporins, ampicillin, erythromycin, aminoglycosides) in large doses, especially with their combinations. Clostridium difficilemultiplies against the background of the death of natural microorganisms living in the colon, under the influence of broad-spectrum antibiotics.
The pathogenesis of pseudomembranous enterocolitis is due to the production of two enterotoxins (A and B) by the pathogen. These toxins have a direct damaging effect on enterocytes, induce the development of an inflammatory response in the intestinal wall and hypersecretion in the colon.
The clinical picture of pseudomembranous enterocolitis is composed of diarrhea (appearing no earlier than 6 weeks of antibiotic therapy), fever and leukocytosis. Further signs of malabsorption syndrome (hypoproteinemia, hypoalbuminemia, edema) are added. In patients with severe diarrhea, pronounced dehydration is often observed. Colonoscopy reveals severe inflammatory changes in the colon mucosa, on which characteristic whitish plaques are located. However, since the latter may be absent, bacteriological examination is necessary to confirm the diagnosis, as well as the determination of toxins A and B in the feces. The most reliable method for detecting Toxin B in feces is to detect its cytopathic effect.
on cell culture, however, the availability of such a study is small. ELISA and latex test for toxins are used as screening tests. Clostridium difficile,contained in feces.
Vancomycin and metronidazole are used to treat pseudomembranous enterocolitis. Oral forms should be preferred. High doses of drugs and a long duration of therapy are indicated, since the disease often recurs.
Prevention of pseudomembranous enterocolitis is the use of rational antibiotic therapy regimens with a decrease in the number of drugs and the duration of their administration, as well as compliance with the rules of aseptic and antiseptic in hospitals.
NSAIDs are one of the most significant causes of ulcerative lesions of the gastric mucosa and duodenal ulcer in the population. The leading factor contributing to the development of NSAID-associated erosions and ulcers of the mucous membrane is considered the blockade of the synthesis of prostaglandins (in particular, prostaglandin E 2) under the influence of these drugs. The likelihood of NSAID-associated ulcers and erosion of the mucous membrane of the stomach and duodenum is maximum in the first 3 months of therapy. In most patients, a subclinical course of the lesion is observed, however, in the presence of the following factors, the appearance of characteristic symptoms and the formation of complications (gastrointestinal bleeding, perforations) are possible. These factors are as follows:
Elderly age.
Taking NSAIDs in large doses and / or their prolonged use.
Concomitant therapy with HA, anticoagulants.
Alcohol abuse.
Infection Helicobacter pylori.
A history of gastric or duodenal ulcer.
Many drugs can cause pancreatitis (tab. 77-3), especially with other predisposing factors (alcohol abuse, gallstone disease, severe hypertriglyceridemia). Medicinal pancreatitis, as a rule, develops within 1 month of taking the drug. Medicinal pancreatitis, as a rule, is an unusually severe course.
Table 77-3.Pancreatitis Medications
Representatives of many classes of drugs can cause a variety of options for liver damage (tab. 77-4). Acute drug damage to the liver with necrosis of large areas of hepatocytes is often accompanied by severe hepatic cell failure and leads to death. The cholestatic variant of drug hepatitis is rarely accompanied by severe clinical manifestations. Some drugs can have a carcinogenic effect on liver tissue, especially in the presence of other predisposing factors, such as alcohol abuse, hepatitis B and C virus infections. In this regard, the appointment of a significant amount of drugs requires monitoring the activity of hepatic transaminases, markers of cholestasis and indicators of synthetic liver function .
Table 77-4.Options for drug damage to the liver and their causes
Kidney damage
Frequency various forms damage to the kidneys induced by drugs in the population is very large. It is believed that any drug has potential nephrotoxicity. There are acute and chronic drug damage to the kidneys.
The following disorders are acute.
One of the most common options is acute tubular necrosis. Among the causes of acute tubular necrosis in the first place are antibacterial drugs, especially aminoglycosides (gentamicin and kanamycin), as well as ampicillin, some cephalosporins and amphotericin B. Semisynthetic penicillins, rifampicin and sulfonamides can also cause acute interstitial nephritis. Acute tubule obstruction is also considered a characteristic side effect of sulfonamides from the kidneys. NSAIDs can cause acute renal failure not only due to acute interstitial nephritis, but also due to impaired renal perfusion as a result of blockages in the synthesis of renal vasodilator prostaglandins.
Among the most common causes of acute deterioration of kidney function include radiopaque substances. The development of acute renal failure with their introduction can be associated both with impaired intrarenal hemodynamics and with the direct toxic effect of contrast agents on the renal tubule epithelium. Prevention of acute tubular nephropathy induced by radiopaque drugs consists in the use of non-ionizing contrasts (iohexol, iopromide), sufficient hydration before the study and prior administration of nondihydropyridine blockers of slow calcium channels (verapamil, diltiazem).
Transient increases in blood potassium and creatinine concentrations are often observed with ACE inhibitors and
angiotensin II receptor blockers in the elderly with advanced atherosclerosis. Their cause is bilateral atherosclerotic stenosis of the renal arteries (ischemic kidney disease), in which these drugs cause further deterioration of renal blood flow. Risk factors for impaired renal function when taking drugs that block the renin-angiotensin-aldosterone system are considered to be the simultaneous use of diuretics or NSAIDs, hypovolemia of any origin, as well as old age and the presence of atherosclerotic lesions of arteries of various locations. For such patients, before prescribing ACE inhibitors or angiotensin II receptor blockers, it is advisable to conduct an ultrasound of the renal arteries in Doppler mode.
Some drugs can cause nephropathy with a primary glomerular lesion. Cases of rapidly progressive glomerulonephritis with prolonged treatment with hydralazine are described. Immunocomplex glomerulonephritis can be induced by penicillamine, gold preparations, lithium.
Among chronic variants of kidney damage, analgesic nephropathy is of the greatest importance. Most NSAIDs are sold over-the-counter, so taking them often becomes uncontrolled.
In the development of analgesic nephropathy, the duration of use and the number of NSAIDs taken are of importance. Patients who consumed up to 30 kg of NSAIDs for 20-30 years are described. The likelihood of analgesic nephropathy is higher when taking combined drugs, including several NSAIDs.
Risk factors for analgesic nephropathy include migraine, old age, chronic joint pain, insomnia, back pain, loneliness, and a feeling of constant malaise. Patients with these conditions often take NSAIDs for prophylactic purposes (prevention of pain).
The pathogenesis of analgesic nephropathy consists of the development of tubulointerstitial nephritis, complemented by damage to the renal papillae with their subsequent calcification. Of leading importance in the development of analgesic nephropathy is the decrease in the intensity of synthesis of renal prostaglandins, accompanied by a deterioration in renal hemodynamics with the development of ischemia of predominantly tubulointerstitial structures.
Analgesic nephropathy is often detected already at the stage of chronic renal failure. The clinical picture of this disease is nonspecific and consists of polyuria, moderate urinary syndrome (erythrocyturia, abacterial leukocyturia). Among the early manifestations include a decrease in the relative density of urine, diagnosed with a Zimnitsky test. With CT, calcification of the papillae is detected. There are 2 groups of diagnostic criteria for analgesic nephropathy. ◊ Big criteria:
♦ daily intake of analgesics for a year or more;
♦ reduction in kidney size, roughness of their contours and calcifications in them during ultrasound;
Prevention of drug disease consists in the rational prescription of drugs with appropriate dose adjustment in patients at risk (elderly, patients with bronchial asthma, chronic renal failure). Information on previously taken drugs requires detailed clarification. The most reliable source of information is medical documentation (discharge epicrisis, outpatient cards). In addition, in the prevention of drug disease, the fight against the independent uncontrolled use of drugs remains important.
The question of theoretical risk that a doctor assumes with any treatment, including drugs, has gained particular popularity in connection with the complications observed in recent years. Professor Georgy Mandrakov says: “A medicine is a symbol of the goals pursued by medicine and the opportunities that it has to achieve these goals.”
Currently, we have a huge number of drugs, we have the most powerful specific drugs, the use of which cures and brings back to life millions of people. However, the widespread use of drugs, the appointment of maintenance and continuous therapies for certain diseases (collagenoses, blood diseases) led to the emergence of many side effects medicines. Before our eyes, diseases that previously were very rare (candidiasis, deep mycoses) are becoming more frequent and new pathological conditions that are still little known appear. So, as you already understood from the introduction, the topic of today's lecture is LB.
Today we must deal with the following questions:
1. definition of the concept, its competence
2. to analyze the etiology and pathogenesis
3. dwell on the features of drug allergies
4. dwell on classification issues
5. disassemble the clinic of LB, damage to individual organs and systems in LB
6. Disassemble the clinic of anaphylactic shock - as the most formidable form of LB
7. methods for diagnosing LB
8. Treatment and prevention of LB
The term LB was first proposed in 1901 by the domestic scientist Arkin Efim Aronovich (he noticed that when rubbing the sulfur-mercury ointment, the patient simultaneously with the rash had severe signs of damage to the whole body (anorexia, asthenia, fever, dyspeptic disorders, etc.) Hence, he naturally expressed the opinion that this disease, which is caused by a medicinal substance and the rash in it, plays the role of only an external manifestation. These drug lesions cannot be called rashes, as it would be wrong to call papulosis Noah, and scarlet fever - an erythematous rash.
The first half of the twentieth century was characterized by the success of chemotherapy. The treatment arsenal included quinoline, benzene derivatives, pyrozole, sulfanilamide preparations, and antibiotics. At the same time, more and more descriptions of complications from their use were accumulating in medical practice. A generalization of these data showed that these complications are completely different in their mechanism of occurrence, pathological changes, and clinical manifestations.
A greater variety of complications of drug therapy did not allow them to lead to a single nosological form, but it was clear that the effect of the drug on the body is a complex biological phenomenon due to many mechanisms, i.e. the concept of side effect medicines.
A.N. Kudrin in 1968 at the 1st International Symposium on Side Effects of Medicines All medical complications are divided into the following groups:
- true side effects of drugs
- toxic effects of drug
- complications associated with sudden withdrawal of a drug
- individual intolerance to the drug
Let us dwell on these concepts.
By the side effect of drugs - understand the undesirable effect of a drug, due to its structure and properties that it has on the body along with its main actions.
Toxic effects of drugs - may be due to overdose, accelerated saturation of the body, the rapid introduction of medium and even minimal doses, insufficient function of the excretory organs (CRF) or a violation of the processes of neutralizing them in the body (with primary liver failure).
Complications due to the rapid withdrawal of drugs (withdrawal syndrome, conditions) - with the rapid withdrawal of some potent drugs, painful symptoms occur that are difficult to tolerate by patients, including withdrawal syndrome. it is characterized by an exacerbation of those symptoms for the elimination of which treatment was carried out.
Individual drug intolerance - is expressed in an unusual perverse reaction of the body to the usual doses of drugs that are harmless to most people. Individual intolerance is a disease of altered body reactivity. Individual intolerance includes idiosyncrasy and an allergic reaction.
Idiosyncrasy is a genetically determined, peculiar response to this medicine when it is first taken. The cause of idiosyncrasy is an insufficient number or low activity of enzymes. For example, a deficiency of the glucose-6-phosphate-DG enzyme in response to certain medications (quinidine, CA drugs, aspirin, pyrazalonic, antibiotics) leads to the development of hemolytic anemia.
Allergic reactions are the most common cause of drug intolerance. The term “allergy” was first coined by the Viennese pediatrician Pirket in 1906. Allergy is now understood to mean the body’s altered sensitivity to the action of this substance, either paraspecifically or because of the hereditary high sensitivity of the body. LB is one of the most significant clinical forms of the body’s allergic reaction to medications.
Continuing the development of the doctrine of LB Landsteiner, which experimentally proved the antigenicity of simple chemical compounds and thereby strengthened the theoretical basis on the unity of the mechanisms of the body's response to substances of non-protein nature. In our country, the nosological outline of LB was substantiated by E. M. Tareev, while at the same time, discussion is still ongoing on the appropriateness of the use of the term LB. Such authors as Ado V.A., Bunin suggest the term LB to denote the entire group of undesirable consequences of active drug therapy, i.e. use it as a group, not a nosological concept.
However, to date, a sufficient number of convincing and indisputable facts have been compiled confirming the nosological outline of this disease (these are the works of Severnova, Nasonova, Semenkov, Mondrakov).
So, one hundred understand by LB?
LB is a peculiar, persistent nonspecific reaction of the body that occurs when using therapeutic or resolving (small) doses of medications and manifests itself in a variety of clinical syndromes. The frequency of LB according to domestic authors is 7-15%, according to foreign authors 18-50%.
Etiology
In fact, any drug can lead to drug allergies. The most common cause of LB is antibiotics (33%). Of these, penicillins account for about 58.7%, BICILLINS 18.5%, streptomycin 15%. In second place are serums and vaccines - 22.8%, for 3 - tranquilizers 13.6%, for 4-hormones - 10%, for 5 - analgesics, SA drugs, in the sixth - antispasmodics - 2.7% and anesthetics - quinine, quinidine, SG, gold preparations, salicylates, vitamins, etc.
The frequency of lesions as a result of pharmacotherapeutic agents, in addition to the medicinal properties of the drug itself and the response of the body when used, depends on many other factors:
- uncontrolled use of drugs by both doctors and patients
- LB most often occurs in a body previously affected by a disease, the underlying disease changes the reactivity of the body, and altered reactivity causes unexpected effects when using drugs.
- an important reason for the development of LB is polypharmacy, which creates the conditions for multivalent sensitization
- nutrition plays an undoubted role, which, when using drugs, can alter the body's reactivity and tolerance to drugs
- age plays an important role in the occurrence of LB. It has long been known for a higher sensitivity of children to barbiturates, salicylates, and in older people to hypertension. This is due to insufficient development in childhood, a decrease in old age - enzyme systems involved in the breakdown and neutralization of certain substances.
- the issue of medicinal genetic lesions and the genetic condition of a number of medicinal lesions is important.
- the degree and rate of sensitization of the body partly depends on the route of administration of drugs. So, local applications and inhalations most often cause sensitization. With the introduction of the introduction of sensitization of the body is less than with vm and vk introductions.
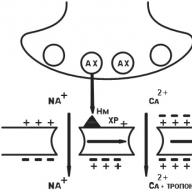
Pathogenesis. As we have already agreed, LB is one of the clinical forms of drug allergy. Most drugs are simple chemical compounds. They are defective antigens (haptens), capable of reacting with antibodies in the body, but they themselves cannot cause their formation. Medicines become full-fledged antibodies only after binding to body tissue proteins. In this case, complex (conjugated) antigens are formed, which cause sensitization of the body. Other drugs, even without splitting, play the role of haptens (levomycetin, erythromycin, diacarb). When reintroduced into the body, these haptens can often bind to formed antibodies or sensitized leukocytes on their own without prior binding to proteins. These areas may be the same for different drugs. They are called common or cross-reactive determinants. Therefore, with sensitization to one drug, allergic reactions to all other drugs that have the same determinant may occur. Medicines with a common determinant:
1. penicillin (natural, semi-synthetic - oxacillin, carbenicillin, cephalosporins), the common determinant for them is the beta-lactam ring. If the patient has a positive allergic reaction to natural penicillins, then he should not be prescribed beta-lactams (zeporin, etc.)
2. novocaine, paraaminosalicylic acid, CA, have a common determinant - aniline (phenylamine)
3. oral hypoglycemic drugs (butamide, bukarban, chlorpropamide), dysuric thiazide (hypothiazide, furosemide), carbanhydrase inhibitors (diacarb) have a common determinant - the benzene-sulfonamide group.
4. antipsychotics (aminosine), antihistamines (diprazine, pipolphene), methylene blue, antidepressants (fluoroacisin), coronary expansion (chloracisin, nanochlozin), antiarrhythmic (ethmosin) and others have a common determinant - phenothiazene group
5. iodine of sodium or potassium, Lugol's solution, iodine-containing contrast agents - iodine.
That is why in most patients polyvalent sensitization to several drugs is observed.
So, for the development of LB (allergies), 3 steps are necessary: \u200b\u200b1. the transformation of the drug into a form that can react with proteins 2. with the body’s proteins to form a complete antigen 3. the body’s immune response to this complex, which has become foreign in the form of antibody formation through the formation of immunoglobulins.
Thus, under the influence of drugs, a specific immunological rearrangement of the body occurs. The following stages of allergic manifestations are distinguished:
1. pre-immunological - the formation of complete (full) allergens (antigens)
2. immunological - an antigen-antibody reaction occurs on the territory of shock organs. This reaction is strictly specific and is caused only by the introduction of a specific allergen.
3. pathochemical - as a result of the formation of the antigen-antibody complex, up to 20 biological active substances (histamine, heparin, serotonin, kinin) are released. The reaction is not specific.
4. pathophysiological - manifested by the pathogenetic effect of biologically active substances on various organs and tissues.
There are allergic reactions of immediate and delayed types. The immediate reaction is the presence of circulating antibodies in the blood. This reaction occurs 30-60 minutes after administration of the drug and is characterized by an acute manifestation: local leukocytosis, eosinophilia. The delayed type reaction is due to the presence of antibodies in the tissues and organs, Yu is accompanied by local lymphocytosis, occurs 1-2 days after taking the drug. The basis of this classification is the time of occurrence of the reaction after administration of the drug. However, it does not cover the entire diversity of allergy manifestations. Therefore, there is a classification of allergic reactions according to the pathogenetic principle (Ado 1970.1978). All allergic reactions are divided into true (actually allergic reactions) and false (pseudo allergic reactions, not immunological). True ones are divided into chimeric (B-dependent) and chitergic (T-dependent), depending on the nature of the immunological mechanism. True allergic reactions have an immunological stage in their development, they falsely do not. Chimeric allergic reactions are caused by the reaction of an antigen with an antibody, the formation of which is associated with B-lymphocytes, kitergic - by the combination of an allergen with sensitized lymphocytes.
Features of drug allergies:
1. its dependence on the type of drug or on the so-called sensitization index. For example, phenethylhydantoin almost always causes allergies (sensitization index 80-90%, in penicillin - 0.3-3%)
2. The development of drug allergy depends on the individual abilities of the body, in which genetic factors have a sore point. For example, children are less likely to suffer from drug allergies than adults. More often, drug allergy develops in patients (i.e., against the background of the underlying disease) than in healthy ones. SLE patients are especially susceptible to drug allergies. Bronchial asthma often develops in individuals with a deficiency of Ig E, prostaglandins, etc.
3. For the development of drug allergies, previous sensitization, especially with protein substances, is of great importance.
4. preferential localization of an allergic reaction, regardless of the method of drug administration: CA, gold - damage the bone marrow, soy heavy metals - toxic-allergic hepatitis.
CLASSIFICATION LB:
according to the severity of occurrence, 2 forms are distinguished:
1. Acute forms · anaphylactic shock · bronchial asthma · acute hemolytic anemia · Quincke’s edema · vasomotor renitis
2. Lingering forms · serum sickness · drug vasculitis · Lyell's syndrome and others.
3 degrees of severity
1. mild (itching, Quincke's edema, urticaria) symptoms disappear 3 days after the appointment of antihistamines
2. moderate severity (urticaria, eczematous dermatitis, erythema multiforme, fever up to 39, poly- or monoarthritis, toxic-allergic myocarditis). Symptoms disappear after 4-5 days, but require the appointment of glucocorticoids in an average dose of 20-40 mg.
3. the severe form is manifested by anaphylactic shock, exfoliative dermatitis, Lyell's syndrome, damage to internal organs (myocarditis with rhythm disorders, nephrotic syndrome) is added. All symptoms disappear after 7-10 days after the combined appointment of not only glucocorticoids, but also immunomodulators, antihistamines.
The early manifestations of LB are very diverse and not very specific, which often makes it difficult to correctly evaluate them. Among them, there is a general deterioration in well-being, malaise, weakness, apathy, usually inexplicable during the underlying disease. there may be headache, dizziness, dyspeptic disorders, etc. the clinical syndromes of LB are also extremely diverse, Polosukhina figuratively speaking, says that the manifestations of LB are diverse and unexpected. Of the many syndromes described, we will focus only on those that have the greatest clinical significance, such as frequent or severe, life-threatening.
Anaphylactic shock
The concept of “anaphylaxis” was first formulated in 1902 by Richet and Porter as an unusual reaction of a dog's body to its repeated administration of an extract from tentacles of acpenib. In 1905, Sakharov described a similar reaction to the reintroduction of horse serum in guinea pigs.
Anaphylaxis is the opposite of protecting the body from the effects of toxic products.
Anaphylactic shock is a type of drug allergy of the immediate type that arose during the reintroduction of the drug into the patient's body. The cause of anaphylactic shock can be all currently used drugs. Most often, anaphylactic shock develops on the introduction of antibiotics (penicillin 0.5-16%). The dose of penicillin caused by shock can be extremely small. For example, a case of shock on traces of penicillin in a syringe remaining in it after a syringe used to administer penicillin to one patient was described, the patient was washed boiled, he was injected with another drug to a patient sensitive to penicillin. Cases of anaphylactic shock on the administration of X-ray contrast agents, relaxants, anesthetics, vitamins, insulin, trypsin, and parathyroid hormones are described. Anaphylactic shock is characterized by a sharp drop in vascular tone, which occurred in direct connection with the administration of the drug and leading to life-threatening circulatory and necrotic changes in the tissues of vital organs - the brain, heart, kidneys, etc.
Anaphylactic drug shock occurs 3-30 minutes after administration of the drug. Clinical signs are diverse. Depending on the severity, 3 degrees of anaphylactic shock are distinguished. The severity of the shock is due to the degree of circulatory disturbance and respiratory function. With a mild course of anaphylactic shock, a short prodromal period of 5-10 minutes is observed, which is characterized by the appearance of itching, urticaria, skin hyperemia, Quincke's edema, laryngeal edema with hoarseness, up to aphonia. Patients have time to complain of chest pain, dizziness, lack of air, blurred vision, numbness of fingers, tongue, lips, abdominal pain, lumbar region.
Objectively: pallor of the skin, cyanosis, filamentous pulse, bronchospasm with distant wheezing, vomiting, loose stools. HELL 6030 - 50
May 11, 2013 Professor I. A. KassirskiiCan we talk about drug sickness?
Indeed, at first glance, this sounds paradoxical. The word “medicine” itself contradicts the notion that a remedy can cause a disease ...
But nevertheless, a drug disease exists, because there is the so-called side effect of drugs.
However, before getting acquainted with a medicinal disease, we immediately make one reservation - we will not think that it is very common and occurs frequently.
We all pay tribute to drugs. It is difficult to imagine how a modern person could undergo surgical operations without painkillers or without antibiotics that bring healing to almost all infectious diseases!
Medicinal substances have been used by people since time immemorial to relieve pain, mental suffering, to treat wounds, like sleeping pills, etc. Initially, therapeutic agents were discovered empirically - they were selected from observations of the plant world, from substances of animal and mineral origin. Their choice was built on the basis of personal experience of people, and attention was drawn to such means that attracted ancient and medieval doctors with their shape, smell, color, taste, strong action (signature).
In those days, action medicinal substances It was tested exclusively in humans, while their dosage was determined on the basis of grossly empirical observations.
It was no accident then that there were poisoning of patients, failures in the treatment of various diseases - manifestations of drug disease.
So, as a result of the inept use of drugs, some doctors, making sure that certain drugs were more dangerous than the diseases that they tried to treat with their help, abandoned the usual methods of treatment. These doctors joined the system of homeopathy, which proclaimed the "law of small doses." But homeopaths were not based on the principles of the scientific method of research, did not consider it necessary to study the complex causes and mechanisms of the development of diseases, and therefore could not give anything substantiated, essential for the treatment of serious diseases. And if homeopaths sometimes bring relief to some patients, it is primarily sick, easily suggestible, with a rapidly depleting nervous system. Homeopathy helps them as a result of psychotherapy or the simultaneous use of conventional medicine.
Since the beginning of the 19th century, drug therapy has become a solid scientific foundation. She uses both the achievements of chemistry and experimental physiological methods for studying the effects of drugs in various dosages on animals. The developed principle of strict individualization in the treatment of patients (to treat the patient, not the disease) contributed to the most rational use of drugs.
While pharmacotherapy is for the most part limited to the average doses that regulate the nervous, cardiovascular, endocrine and other systems of the body, with antibacterial therapy, to suppress the infectious onset, one has to resort to increased doses of drugs and use these medications for a long time. So, for example, chronic blood poisoning, tuberculosis, syphilis and other diseases are treated with chemo drugs for a long time. This sometimes leads to a small toxic effect of antibiotics.
Current use of drugs
 Currently, all drugs are used on the basis of an accurate clinical study of diseases, therefore, almost all drugs produced by pharmacies according to prescriptions of doctors and in the free market are completely safe. But it is very important to observe rational doses of their use recommended by doctors.
Currently, all drugs are used on the basis of an accurate clinical study of diseases, therefore, almost all drugs produced by pharmacies according to prescriptions of doctors and in the free market are completely safe. But it is very important to observe rational doses of their use recommended by doctors.
This is confirmed by simple statistics.
During the day, millions of people take various medications at home and in hospitals. Some medications, such as headaches, constipation, sedatives, light heart drops, external disinfectants, are part of everyday life and certainly help people live and work. More serious medications that require medical advice are also used on a large scale. And if we ask: are there often cases of the so-called drug disease in those taking medications, we must answer negatively: No, very rarely!
However, doctors, naturally, strive to ensure that these cases are not observed at all, because a drug disease can cause a person great harm. And in order to know how to deal with it, you need to find out why it happens.
Causes of drug sickness?
The cause of a drug disease may be primarily an increase against the norm of a single dose of a drug, the so-called overdose. We give only one example: arsenic in small doses has a therapeutic value, while in large doses it destroys the body.
For the occurrence of a drug disease, the accumulation of the action of a particular drug in the body - the so-called cumulation - of irrational long-term use of a medicinal product is important.
An example of the latter is the cumulative effect bromine.
With prolonged use, a runny nose may occur, rashes on the skin appear, memory weakens, general well-being also worsens. It is clear that the drug should be canceled in a timely manner. But doctors can easily cope with such manifestations of a drug disease, they are known, they can be foreseen and timely prevented. But what if the drug disease — the toxic effect of various drugs — is sharply manifested individually in a patient?
 So, after application streptomycin severe dizziness or hearing loss may occur. This is because streptomycin has a particular toxic effect on the nerves of the inner ear.
So, after application streptomycin severe dizziness or hearing loss may occur. This is because streptomycin has a particular toxic effect on the nerves of the inner ear.
However, it must be emphasized that this complication is very rare, only in 1-2 percent of cases, and is temporary. All these phenomena usually disappear as soon as the use of streptomycin is stopped.
Therefore, doctors who are tasked with curing, for example, a serious illness such as tuberculosis, practically neglect the danger of the possible occurrence of this temporary complication.
But in some patients, this complication is so intense that doctors even have to cancel streptomycin.
The above examples emphasize how useful it is to know and study drug disease. This knowledge helps doctors and patients to avoid the development of serious complications associated with drug therapy.
It is especially important to remember the toxic effects of antibacterial drugs used to treat certain infections. These funds, as we have already said, have to be used in large enough doses and often for a long time. Therefore, doctors, without waiting for even the smallest toxic effect, take precautionary measures in advance. They carefully monitor the reaction of the blood of patients, the temperature, the state of the nervous system.
In the prevention of drug illness, the intermittent treatment method used by doctors is of particular importance, this is the surest means. It is useful from two points of view: firstly, because the body itself rests for a while from the toxic effect of the drug; secondly, interruptions in treatment have a positive effect on overcoming the infectious onset. Indeed, with prolonged use of antibacterial drugs, microbes seem to get used to them, their resistance to drugs develops. However, after a certain interval, the microbes again become sensitive to antibacterial drugs, and the latter gain their initial healing power.
It is more difficult to account for and prevent the form of a drug disease associated with a particular increased individual sensitivity of the patient’s body to a particular drug, and often quite innocent, which can be sold in pharmacies even without a doctor’s prescription.
Hypersensitivity - Allergy
 Hypersensitivity of this kind - allergy, this is a special innate or acquired property of the body to respond with painful reactions to certain agents that are introduced into the body in normal doses.
Hypersensitivity of this kind - allergy, this is a special innate or acquired property of the body to respond with painful reactions to certain agents that are introduced into the body in normal doses.
There are many examples of such allergies.
Allergic reactions to drugs are characterized by changes in the blood; with intolerance to streptocide, sulfazole, antibiotics, often there is severe urticaria or eczema-like skin damage, swelling of the face, itching in the perineum, etc.
The development of fungi after antibiotics
There is another form of drug disease caused by fungi. What does it depend on? In the treatment with antibiotics, as a rule, there is a suppression of some common non-pathogenic microbes that inhabit the intestines, and in this connection activation of yeast fungi, which always inhabit the digestive tract, respiratory tract, and skin. As a result, a fungal disease develops, the so-called candidiasis, or candidiasis.
What conclusions should be drawn from the above facts?
It must, of course, be remembered that in the vast, overwhelming majority of drugs that are administered as prescribed by doctors or purchased in pharmacies without prescriptions, they help a person.
Antibiotics have led mankind to victory over many diseases - epidemic meningitis, pneumonia, tuberculosis, tuberculous meningitis, etc. Meanwhile, not so long ago, the diagnosis of many of the diseases just listed meant death - quick from plague and meningitis and almost inevitable, sooner or later, from tuberculosis.
However, the treatment of diseases has its own laws. Doctors know these laws well. But patients should also be aware of the side effects of drugs, of the possibility of a drug disease in connection with this, in order to prevent even its minimal danger.