Pathophysilogy of histamine andH 1histamine receptors
Histamine and its effects mediated through H 1 receptors
Stimulation of H 1 receptors in humans leads to an increase in smooth muscle tone, vascular permeability, the appearance of itching, slowing of atrioventricular conduction, tachycardia, activation of the vagus nerve branches that innervate the airways, increase the level of cGMP, increase the formation of prostaglandins, etc. In the table. 19-1 localization shown H 1receptors and the effects of histamine mediated through them.
Table 19-1.Localization H 1receptors and the effects of histamine mediated through them
The role of histamine in the pathogenesis of allergies
Histamine has a leading role in the development of atopic syndrome. In allergic reactions mediated through IgE, a large amount of histamine enters the tissues from mast cells, causing the occurrence of the following effects through exposure to H 1 receptors.
In the smooth muscles of large vessels, bronchi and intestines, the activation of H 1 receptors causes a change in the conformation of the Gp protein, which, in turn, leads to the activation of phospholipase C, which catalyzes the hydrolysis of inositol diphosphate to inositol triphosphate and diacylglycerols. An increase in the concentration of inositol triphosphate leads to the opening of calcium channels in the EPR ("calcium depot"), which causes the release of calcium into the cytoplasm and an increase in its concentration inside the cell. This leads to activation of the calcium / calmodulin-dependent kinase of myosin light chains and, accordingly, to the reduction of smooth muscle cells. In an experiment, histamine causes a biphasic contraction of the smooth muscles of the trachea, consisting of a rapid phase contraction and a slow tonic component. It was shown in experiments that the fast phase of contraction of these smooth muscles depends on intracellular calcium, and the slow one depends on the entry of extracellular calcium through slow calcium channels that are not blocked by calcium antagonists. Acting through the H 1 receptors, histamine causes a reduction in the smooth muscles of the respiratory tract, including the bronchi. In the upper respiratory tract, there is more histamine H 1 receptors than in the lower, which is significant in the severity of bronchospasm in bronchioles during the interaction of histamine with these receptors. Histamine induces obstruction of the bronchi as a result of direct influence to the smooth muscles of the respiratory tract, reacting with histamine H 1 receptors. In addition, through H 1 receptors, histamine increases the secretion of fluid and electrolytes in the airways and causes increased mucus production and edema of the airways. Patients with bronchial asthma are 100 times more sensitive to histamine than healthy individuals when conducting a histamine provocation test.
In the endothelium of small vessels (post-capillary venules), the vasodilating effect of histamine is mediated through the H 1 receptors in allergic reactions of the reagin type (through the H 2 receptors of smooth muscle cells of the venules, via the adenylate cyclase pathway). Activation of the H 1 receptors leads (along the phospholipase pathway) to an increase in the intracellular level of calcium, which, together with diacylglycerol, activates the phospholipase A 2, causing the following effects.
Local release of endothelium-relaxing factor. It penetrates into neighboring smooth muscle cells and activates guanylate cyclase. As a result, the concentration of cGMP activating cGMP-dependent protein kinase increases, which leads to a decrease in intracellular calcium. With a simultaneous decrease in calcium level and an increase in cGMP level, smooth muscle cells of postcapillary venules relax, which leads to the development of edema and erythema.
When phospholipase A2 is activated, the synthesis of prostaglandins, mainly the prostacyclin vasodilator, increases, which also contributes to the formation of edema and erythema.
Classification of antihistamines
There are several classifications of antihistamines (histamine H 1 receptor blockers), although not one is generally accepted. According to one of the most popular classifications, antihistamines at the time of creation are divided into drugs of the I and II generation. I generation drugs are also called sedatives (by the dominant side effect), in contrast to non-sedative drugs of the second generation. The first generation antihistamines include: diphenhydramine (diphenhydramine *), promethazine (diprazine *, pipolfen *), clemastine, chloropyramine (suprastin *), chifenadine (phencarol *), sequifenadine (bicarfen *). II generation antihistamines: terfenadine *, astemizole *, cetirizine, loratadine, ebastine, cyproheptadine, oxatomide * 9, azelastine, acrivastine, mebhydroline, dimetinden.
At present, it is customary to isolate the III generation of antihistamines. It includes fundamentally new drugs - active metabolites, which are characterized in addition to high antihistamine activity, the absence of a sedative effect and the cardiotoxic effect characteristic of second-generation drugs. Fexofenadine (telfast *), desloratadine are referred to the third generation of antihistamines.
In addition, the chemical structure of antihistamines is divided into several groups (ethanolamines, ethylenediamines, alkylamines, derivatives of alfacarbolin, quinuclidine, phenothiazine *, piperazine * and piperidine *).
The mechanism of action and the main pharmacodynamic effects of antihistamines
Most used antihistamines has specific pharmacological properties, which characterizes them as a separate group. These include the following effects: antipruritic, decongestion, antispastic, anticholinergic, antiserotonin, sedative and local anesthetizing, as well as the prevention of histamine-induced bronchospasm.
Antihistamines are antagonists of histamine H 1 receptors, and their affinity for these receptors is significantly lower than that of histamine (Table 19-2). That is why these drugs are not able to displace the histamine associated with the receptor, they only block unoccupied or released receptors.
Table 19-2.Comparative effectiveness of antihistamines according to the degree of blockade H 1histamine receptors
 Accordingly, blockers H 1histamine receptors are most effective in preventing allergic reactions immediate type, and in case of a developed reaction, the release of new portions of histamine is prevented. The binding of antihistamines to receptors is reversible, and the number of blocked receptors is directly proportional to the concentration of the drug at the receptor location.
Accordingly, blockers H 1histamine receptors are most effective in preventing allergic reactions immediate type, and in case of a developed reaction, the release of new portions of histamine is prevented. The binding of antihistamines to receptors is reversible, and the number of blocked receptors is directly proportional to the concentration of the drug at the receptor location.
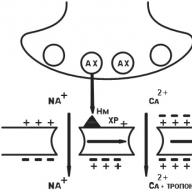
The molecular mechanism of action of antihistamines can be represented in the form of a scheme: blockade of the H 1 receptor — blockade of the phosphoinositide pathway in the cell — blockade of the effects of histamine. The binding of drugs to the histamine H 1 receptor leads to receptor blockade, i.e. interferes with the binding of histamine to the receptor and the launch of the cascade in the cell along the phosphoinositide pathway. Thus, the binding of antihistamine drugs to the receptor causes a slowdown in the activation of phospholipase C, which leads to a decrease in the formation of inositol triphosphate and diacylglycerol from phosphatidylinositol, and, as a result, the calcium release from intracellular depots slows down. A decrease in the release of calcium from intracellular organelles into the cytoplasm in various types of cells leads to a decrease in the proportion of activated enzymes that mediate the effects of histamine in these cells. In the smooth muscles of the bronchi (as well as the gastrointestinal tract and large vessels), the activation of calcium-calmodulin-dependent kinase of myosin light chains slows down. This prevents histamine-induced smooth muscle contraction, especially in patients with asthma. However, with bronchial asthma, the concentration of histamine in the lung tissue is so high that modern N 1 -blockers are not able to block the effects of histamine on the bronchi by this mechanism. In the endothelial cells of all postcapillary venules, antihistamines inhibit the vasodilating effect of histamine (direct and via prostaglandins) in local and generalized allergic reactions (histamine also acts through the histamine H 2 receptors of smooth muscle cells
venule along the adenylate cyclase pathway). The blockade of histamine H 1 receptors in these cells prevents an increase in intracellular calcium levels, ultimately slowing down the activation of phospholipase A2, which leads to the development of the following effects:
Slowing down the local release of the endothelium-relaxing factor, which penetrates into the neighboring smooth muscle cells and activates guanylate cyclase. Inhibition of guanylate cyclase activation decreases the concentration of cGMP, then the fraction of activated cGMP-dependent protein kinase decreases, which prevents the decrease in calcium levels. At the same time, normalization of calcium and cGMP prevents the relaxation of smooth muscle cells of postcapillary venules, that is, it prevents the development of edema and erythema caused by histamine;
Reducing the activated fraction of phospholipase A2 and reducing the synthesis of prostaglandins (mainly prostacyclin), vasodilation is blocked, which prevents the occurrence of edema and erythema caused by histamine by its second mechanism of action on these cells.
Based on the mechanism of action of antihistamines, these drugs should be prescribed in order to prevent allergic reactions of the reagin type. The appointment of these drugs with an allergic reaction that has developed is less effective, since they do not eliminate the symptoms of an allergy that have developed, but they prevent their appearance. Histamine H 1 receptor blockers prevent the reaction of smooth muscle of the bronchi to histamine, reduce itching, and prevent the expansion of small vessels and their permeability mediated by histamine.
Pharmacokinetics of antihistamines
The pharmacokinetics of first-generation histamine H 1 receptor blockers is fundamentally different from the pharmacokinetics of second-generation drugs (Table 19-3).
The penetration of antihistamines of the first generation through the BBB leads to the appearance of a pronounced sedative effect, which is considered a significant drawback of drugs of this group and significantly limits their use.
II generation antihistamines are characterized by relative hydrophilicity and therefore do not penetrate the BBB and, therefore, do not cause a sedative effect. It is known that 80% of astemizole * is excreted 14 days after the last dose, and terfenadine * - after 12 days.
Pronounced ionization of diphenhydramine at physiological pH values \u200b\u200band active non-specific interaction with serum
oral albumin determines its effect on the histamine H 1 receptors located in various tissues, which leads to quite pronounced side effects of this drug. In blood plasma, the maximum concentration of drugs is determined 4 hours after its administration and is equal to 75-90 ng / l (at a dose of 50 mg). The elimination half-life is 7 hours.
The peak concentration of clemastine is achieved 3-5 hours after a single oral dose of 2 mg. The elimination half-life is 4-6 hours.
Terfenadine * is rapidly absorbed by ingestion. Metabolized in the liver. The maximum concentration in the tissues is determined after 0.5-1-2 hours after taking the drug, the half-life is
The maximum level of unchanged astemizole * is noted within 1-4 hours after taking the drug. Food reduces astemizole * absorption by 60%. The peak concentration of drugs in the blood with a single oral administration occurs after 1 hour. The half-life of the drug is 104 hours. Hydroxyastemizole and norastemizole are its active metabolites. Astemizole * crosses the placenta, in small amounts into breast milk.
The maximum concentration of oxatomide * in the blood is determined 2-4 hours after administration. The elimination half-life is 32-48 hours. The main metabolic pathway is aromatic hydroxylation and oxidative dealkylation on nitrogen. 76% of the absorbed drug is attached to plasma albumin, from 5 to 15% is excreted in breast milk.
Table 19-3.Pharmacokinetic parameters of some antihistamines
 The maximum level of cetirizine in the blood (0.3 μg / ml) is determined 30-60 minutes after taking this drug at a dose of 10 mg. Renal
The maximum level of cetirizine in the blood (0.3 μg / ml) is determined 30-60 minutes after taking this drug at a dose of 10 mg. Renal
the clearance of cetirizine is 30 mg / min, the half-life is about 9 hours. The drug stably binds to blood proteins.
The peak concentration of acrivastine in plasma is reached 1.4-2 hours after administration. The half-life is 1.5-1.7 hours. Two-thirds of the drug in unchanged form is excreted by the kidneys.
Loratadine is well absorbed in the digestive tract and after 15 minutes it is determined in the blood plasma. Food does not affect the degree of absorption of drugs. The half-life of the drug is 24 hours.
1st generation antihistamines
For blockers of H 1 receptors of histamine I generation, some features are characteristic.
Sedative action.Most antihistamines of the first generation, easily dissolving in lipids, penetrate well through the BBB and bind to the H 1 receptors of the brain. Apparently, a sedative effect develops with the blockade of central serotonin and m-cholinergic receptors. The degree of development of a sedative effect varies from moderate to severe and is enhanced when combined with alcohol and psychotropic drugs. Some drugs in this group are used as sleeping pills (doxylamine). Rarely, instead of sedation, psychomotor agitation occurs (more often in moderate therapeutic doses in children and in high toxic doses in adults). Due to the sedative effect of drugs, they can not be used during the period of work requiring attention. All blockers of H 1 receptors of histamine I generation potentiate the effects of sedative and hypnotic drugs, narcotic and non-narcotic analgesics, monoamine oxidase inhibitors and alcohol.
Anxiolytic effectinherent in hydroxyzine. This effect, possibly, arises due to the suppression of the activity of certain parts of the subcortical formations of the brain by hydroxyzine.
Atropine-like action.This effect is associated with the blockade of m-cholinergic receptors, most characteristic of ethanolamines and ethylenediamines. Dry mouth, urinary retention, constipation, tachycardia, and visual impairment are characteristic. In non-allergic rhinitis, the effectiveness of these drugs increases due to the blockade of m-cholinergic receptors. However, it is possible to increase bronchial obstruction due to an increase in sputum viscosity, which is dangerous for bronchial asthma. Generation I histamine H 1 receptor blockers can exacerbate glaucoma and cause acute urinary retention in prostate adenoma.
Antiemetic and anti-pumping action.These effects may also be associated with a central m-anticholinergic action of these drugs. Diphenhydramine, promethazine, cyclizine *, mekli-
zine * reduce the stimulation of the vestibular receptors and inhibit the function of the maze, and therefore can be used for motion sickness.
Some histamine H 1 receptor blockers reduce the symptoms of parkinsonism due to a blockade of central m-cholinergic receptors.
Antitussive effect.Most characteristic of diphenhydramine, it is realized due to the direct action on the cough center in the medulla oblongata.
Antiserotonin action.Cyproheptadine possesses it the most, so it is used for migraines.
The effect of blockade of a 1-adrenaline receptors with peripheral vasodilation is especially characteristic of phenothiazine preparations. This can lead to a transient decrease in blood pressure.
Local anestheticthe action is characteristic of most drugs in this group. The effect of local anesthesia of diphenhydramine and promethazine is stronger than that of novocaine *.
Tachyphylaxis- a decrease in the antihistamine effect with prolonged use, confirming the need for alternating drugs every 2-3 weeks.
Pharmacodynamics of H 1 blockers of histamine I generation
All blockers of the H 1 receptors of histamine I generation I are lipophilic and, in addition to the H 1 receptors of histamine, also block m-cholinergic receptors and serotonin receptors.
When prescribing histamine receptor blockers, the phase course of the allergic process must be considered. Histamine H 1 blockers of histamine receptors should be used mainly for the prevention of pathogenetic changes in case of a patient’s expected meeting with an allergen.
1st generation histamine H 1 receptor blockers do not affect histamine synthesis. In high concentrations, these drugs can cause mast cell degranulation and histamine exit from them. Histamine H 1 receptor blockers are more effective in preventing the action of histamine than in eliminating the effects of its effects. These drugs inhibit the reaction of smooth muscles of the bronchi to histamine, reduce itching, prevent the increase in vascular histamine expansion and increase their permeability, and reduce the secretion of endocrine glands. It is proved that blockers of H 1 receptors of histamine I generation have a direct bronchodilating effect, and most importantly, they prevent the release of histamine from mast cells and blood basophils, which is considered the basis for the use of these drugs
as prophylactic agents. In therapeutic doses, they do not significantly affect the cardiovascular system. With forced intravenous administration, they can cause a decrease in blood pressure.
Blockers of H 1 receptors of histamine I generation are effective in the prevention and treatment of allergic rhinitis (efficiency about 80%), conjunctivitis, pruritus, dermatitis and urticaria, angioedema, some types of eczema, anaphylactic shock, with edema caused by hypothermia. First-generation histamine H 1 receptor blockers are used in conjunction with sympathomimetics in allergic rhinorrhea. Derivatives of piperazine * and phenothiazine * are used to prevent nausea, vomiting and dizziness caused by sudden movements, with Meniere's disease, with vomiting after anesthesia, with radiation sickness and morning vomiting in pregnant women.
Local application of these drugs takes into account their antipruritic, anesthetic and analgesic effects. It is not recommended to use them for a long time, since many of them are capable of causing hypersensitivity and have a photosensitizing effect.
Pharmacokinetics of histamine I-blockers of the 1st generation
Blockers of H 1 receptors of histamine I generation differ from second-generation drugs in the short duration of action with a relatively rapid onset of clinical effect. The effect of these drugs arises, on average, 30 minutes after taking the drug, reaching a peak within 1-2 hours. The duration of action of the first generation antihistamines is 4-12 hours. The short duration of the clinical effect of the first generation antihistamines is associated, first of all, with the fast metabolism and excretion by the kidneys.
Most of the first-generation histamine H 1 receptor blockers are well absorbed in the digestive tract. These drugs penetrate the BBB, the placenta, and also pass into breast milk. The highest concentrations of these drugs are found in the lungs, liver, brain, kidneys, spleen and muscles.
Most blockers of H 1 receptors of histamine I generation are metabolized in the liver by 70-90%. They induce microsomal enzymes, which when prolonged use can reduce their therapeutic effect, as well as the effect of other drugs. The metabolites of many antihistamines are excreted within 24 hours with urine and only small amounts are unchanged.
Side effects and contraindications
Side effects caused by blockers of H 1 receptors of histamine I generation are presented in table. 19-4.
Table 19-4.Undesirable drug reactions of antihistamines of the first generation
 Large doses of histamine H 1 receptor blockers can cause agitation and seizures, especially in children. With these symptoms, barbiturates cannot be used, as this will cause an additive effect and significant inhibition of the respiratory center. Cyclizine * and chlorocyclisin * have teratogenic effects, so they can not be used for vomiting in pregnant women.
Large doses of histamine H 1 receptor blockers can cause agitation and seizures, especially in children. With these symptoms, barbiturates cannot be used, as this will cause an additive effect and significant inhibition of the respiratory center. Cyclizine * and chlorocyclisin * have teratogenic effects, so they can not be used for vomiting in pregnant women.
Drug Interactions
1st generation histamine H 1 receptor blockers potentiate the effects of narcotic analgesics, ethanol, sleeping pills, tranquilizers. May enhance the action of CNS stimulants in children. With prolonged use, these drugs reduce the effectiveness of steroids, anticoagulants, phenylbutazone (butadione *) and other drugs that are metabolized in the liver. Their combined use with anticholinergics can lead to an excessive increase in their effects. MAO inhibitors enhance the effect of antihistamines. Some first-generation drugs potentiate the effects of adrenaline and norepinephrine on the cardiovascular system. Blockers of the H 1 receptors of histamine I generation are prescribed for the prevention of clinical symptoms of allergies, in particular, rhinitis, often accompanying atopic bronchial asthma, for the relief of anaphylactic shock.
Antihistamines medicines II and III generations
The second generation drugs include terfenadine *, astemizole *, cetirizine, mekvipazin *, fexofenadine, loratadine, ebastin, and the third generation of histamine H 1 receptor blockers - fexofenadine (telfast *).
The following features of the blockers of H 1 receptors of histamine II and III generations can be distinguished:
High specificity and high affinity for histamine H 1 receptors with no effect on serotonin and m-cholinergic receptors;
The rapid onset of the clinical effect and duration of action, which is usually achieved by a high degree of protein binding, cumulation of the drug or its metabolite in the body and delayed elimination;
Minimal sedation when using drugs in therapeutic doses; some patients may experience moderate drowsiness, which is rarely the cause of drug withdrawal;
Lack of tachyphylaxis with prolonged use;
The ability to block potassium channels of the cells of the conduction system of the heart, which is associated with an extension of the interval Q-Tand violation of the rhythm of the heart (ventricular tachycardia of the pirouette type).
In the table. 19-5 presents a comparative characteristic of some blockers of H 1 receptors of histamine II generation.
Table 19-5.Comparative characteristics of blockers of H 1 receptor histamine II generation
 The end of the table. 19-5
The end of the table. 19-5
 Pharmacodynamics of blockers of the H-receptors of histamine II generation
Pharmacodynamics of blockers of the H-receptors of histamine II generation
Astemizole * and terfenadine * do not have choline and β-blocking activity. Astemizole * blocks α-adreno- and serotonin receptors only in large doses. Gene II histamine H 1 receptor blockers have a weak therapeutic effect in bronchial asthma, since not only histamine, but also leukotrienes, platelet activation factor, cytokines and other mediators causing the development of the disease affect the smooth muscles of the bronchi and bronchial glands. The use of only histamine H 1 receptor blockers does not guarantee complete relief of bronchospasm of allergic genesis.
Pharmacokinetics of the blockers of H 1 receptors of histamine II generationAll II-generation histamine H 1 receptor blockers act for a long time (24-48 hours), and the time for the development of the effect is small - 30-60 minutes. About 80% of astemizole * is excreted 14 days after the last dose, and terfenadine * - after 12 days. The cumulative effect of these drugs, proceeding without changing the functions of the central nervous system, allows them to be widely used in outpatient practice in patients with pollinosis, urticaria, rhinitis, neurodermatitis, etc. II generation histamine H 1 receptor blockers are used in the treatment of patients with bronchial asthma with individual dose selection.
For blockers of H 1 receptors of histamine of the second generation, the cardiotoxic effect due to bloc
potassium channels of cardiomyocytes and expressed by lengthening the interval Q-Tand arrhythmia on an electrocardiogram.
The risk of this side effect increases with the combination of antihistamines with inhibitors of the cytochrome P-450 3A4 isoenzyme (appendix 1.3): antifungal drugs (ketoconazole and intraconazole *), macrolides (erythromycin, oleandomycin and clarithromycin), antidepressin-ferromytoxin and erythroxetinomethrin-fluoromethrin-etromethrin-fluoromethinoxinetromethinoxin-etromethrin , with the use of grapefruit juice, as well as in patients with severe impaired liver function. The combined use of the above macrolides with astemizole * and terfenadine * in 10% of cases leads to a cardiotoxic effect associated with lengthening the interval Q-T.Azithromycin and dirithromycin * are macrolides that do not inhibit the 3A4 isoenzyme, and, therefore, do not cause an extension of the interval Q-Twhile taking second-generation histamine H 1 receptors with blockers.
I.V. Smolenov, N.A. Smirnov
Department of Clinical Pharmacology, Volgograd Medical Academy
In recent years, there has been a significant increase in the frequency and severity of allergic diseases and reactions. This is due to environmental pollution, an increase in ozone concentration, and a change in people's lifestyle. The costs of treating patients with atopic asthma, allergic rhinitis, and atopic dermatitis also increase significantly. These conditions, as a rule, are not life-threatening, but require active therapeutic intervention, which should be effective, safe and well tolerated by patients.
A significant role in the development of allergic reactions is played by mediators of various chemical structures - biogenic amines (histamine, serotonin), leukotrienes, prostaglandins, kinins, chemotoxic factors, cationic proteins, etc. In recent years, new drugs with anti-mediating effects have been synthesized and tested - antagonists of leukotriene receptors (zafirlukast, montelukast), 5-lipoxygenase inhibitors (zeliuton), antichemotoxic agents. However, drugs with an antihistamine effect have found the widest application in clinical practice.
The feasibility of using antihistamines for various allergic diseases (urticaria, atopic dermatitis, allergic rhinitis and conjunctivitis, allergic gastropathy) is due to a wide range of histamine effects. This mediator is able to affect the respiratory tract (causing swelling of the nasal mucosa, bronchospasm, mucus hypersecretion), skin (itching, blister-hyperemic reaction), gastrointestinal tract (intestinal colic, stimulation of gastric secretion), cardiovascular system (expansion of capillary blood vessels, increased vascular permeability, hypotension, heart rhythm disturbance), smooth muscles (spasm).
The first drugs competitively blocking histamine receptors were introduced into clinical practice in 1947. Drugs that compete with histamine at the level of H 1 receptors of target organs are classified as H 1 blockers, H 1 receptor blockers, or antihistamines. Medicines of this class have a weak effect on H 2 and H 3 receptors.
Antihistamines inhibit the symptoms associated with the endogenous release of histamine, inhibit the development of hyperreactivity, but do not affect the sensitizing effect of allergens and do not affect the infiltration of mucous membranes by eosinophils. In the case of late administration of antihistamines, when the allergic reaction is already significantly expressed and most histamine receptors are associated, the clinical effectiveness of these drugs is low.
In recent decades, drugs have been created that can not only block H 1 receptors, but also have an additional effect on the processes of allergic inflammation. The presence of additional pharmacodynamic effects in modern antihistamines served as the basis for their separation into three main generations (Table 1).
The effectiveness of first-generation antihistamines in the treatment of allergic rhinoconjunctivitis, urticaria and other allergic diseases has been established for a long time. However, although all these drugs quickly (usually within 15-30 minutes) alleviate the symptoms of allergies, most of them have a pronounced sedative effect and can cause unwanted reactions at recommended doses, as well as interact with other drugs and alcohol. The sedative effect is due to the ability of antihistamines of the first generation to penetrate the blood-brain barrier. Their use can also cause the occurrence of gastrointestinal manifestations: nausea, vomiting, constipation and diarrhea.
Currently, 1st generation antihistamines are used mainly for the relief of acute allergic reactions in situations where the reactions of the early phase of allergic inflammation predominate, and the presence of an additional anti-allergic effect is not mandatory:
acute allergic urticaria;
anaphylactic or anaphylactoid shock, allergic Quincke edema (parenterally, as an additional tool);
prevention and treatment of allergic and pseudo-allergic reactions caused by drugs;
seasonal allergic rhinitis (episodic symptoms or duration of exacerbations<2 недель);
acute allergic reactions to foods;
serum sickness.
Some first-generation antihistamines have a pronounced anticholinergic activity, as well as the ability to block muscarinic cholinergic receptors. Due to this, 1st generation drugs can also be effective in the following situations:
|
With ARVI(drugs with anticholinergic effect have a "drying" effect on the mucous membranes): |
|
Pheniramine ( Avil); Fervex). Promethazine ( Pipolphen, Diprazin); Paracetamol + Dextromethorphan ( Coldrex nite). Chloropyramine ( Suprastin). Chlorphenamine; Paracetamol + ascorbic acid ( Antigrippin); Paracetamol + Pseudoephedrine ( Theraflu, Antiflu); Biclotimol + Phenylephrine ( Hexapneumine); Phenylpropanolamine ( CONTAC 400); + phenylpropanolamine + acetylsalicylic acid (HL-cold). Diphenhydramine ( Dimimedrol). |
|
For cough suppression: |
|
Diphenhydramine ( Dimimedrol) Promethazine ( Pipolphen, Diprazin) |
|
For the correction of sleep disorders(improve falling asleep, depth and quality of sleep, but the effect lasts no more than 7-8 days): |
|
Diphenhydramine ( Dimimedrol); Paracetamol ( Efferalgan nightcare). To stimulate appetite: Cyproheptadine ( Peritol); Astemizole ( Hismanal). |
|
For the prevention of nausea and dizziness due to labyrinthitis or Meniere's disease, as well as to reduce the manifestations of motion sickness: |
|
Diphenhydramine ( Dimimedrol) Promethazine ( Pipolphen, Diprazin) |
|
For the treatment of pregnant vomiting: |
|
Diphenhydramine ( Dimimedrol) |
|
To potentiate the effects of analgesics and local anesthetics (sedation, a component of lytic mixtures): |
|
Diphenhydramine ( Dimimedrol) Promethazine ( Pipolphen, Diprazin) |
|
For the treatment of small cuts, burns, insect bites(the effectiveness of topical use of drugs is not strictly proven, it is not recommended to use\u003e 3 weeks due to an increased risk of local irritation): Bamipin ( Soventol). |
The advantages of the 2nd generation antihistamines include a wider range of indications for use (bronchial asthma, atopic dermatitis, hay fever, allergic rhinitis) and the presence of additional anti-allergic effects: the ability to stabilize mast cell membranes, suppress the PAT-induced accumulation of eosinophils in the airways.
However, the idea of \u200b\u200bthe clinical efficacy of 2nd generation antihistamines in the treatment of bronchial asthma and atopic dermatitis is based on a small number of uncontrolled studies. Ketotifen was not registered in a number of countries (in particular in the USA), since convincing data on its effectiveness were not provided. The action of the drug develops rather slowly (within 4-8 weeks), and the pharmacodynamic effects of the 2nd generation drugs are proved only mainly in vitro. Among side effects ketotifen recorded sedative effect, dyspeptic symptoms, increased appetite, as well as thrombocytopenia.
Recently, 3rd generation antihistamines have been developed with significant selectivity, acting only on peripheral H 1 receptors. These drugs do not pass the blood-brain barrier and therefore do not have side effects from the central nervous system. In addition, modern antihistamines have some significant additional anti-allergic effects: they reduce the expression of adhesion molecules (ICAM-1) and suppress eosinophil-induced secretion of IL-8, GM-CSF and sICAM-1 from epithelial cells, reduce the severity of allergen-induced bronchospasm, reduce the phenomenon of bronchial hyperreactivity.
The use of 3rd generation antihistamines is more justified during long-term therapy of allergic diseases, in the genesis of which mediators of the late phase of allergic inflammation play a significant role:
year-round allergic rhinitis;
seasonal allergic rhinitis (conjunctivitis) with a duration of seasonal exacerbations\u003e 2 weeks;
chronic urticaria;
atopic dermatitis;
allergic contact dermatitis;
early atopic syndrome in children.
The pharmacokinetic properties of antihistamines vary significantly. Most 1st generation drugs have a short duration of action (4-12 hours) and require multiple dosing. Modern antihistamines have a long duration of action (12-48 hours), which allows them to be prescribed 1-2 times a day. The maximum elimination half-life has astemizole (about 10 days), which inhibits skin reactions to histamine and allergens for 6-8 weeks.
Serious cardiotoxic side effects in the form of severe cardiac arrhythmias have been described for two 3rd generation antihistamines (terfenadine and astemizole). The likelihood of developing these side effects increases with the simultaneous administration of drugs with macrolides (erythromycin, oleandomycin, azithromycin, clarithromycin), antifungal agents (ketocanozole and intracanozole), antiarrhythmics (quinidine, novocainamide, disopyramide), some antidepressant diseases, and also liver disease patients and hyperkalemia. If you need the simultaneous use of terfenadine or astemizole with the above groups of drugs, preference is given to antifungal agents fluconazole (diflucan) and terbenafine (lamisil), antidepressants paroxetene and sertraline, antiarrhythmics and antibiotics of other groups. The characteristics of modern antihistamines, the features of their dosage and the comparative cost of treatment are shown in table 2.
The degree of affinity of the “old” and “new” preparations for the H 1 histamine receptors is approximately the same. Therefore, the choice of the drug is due to the exchange rate of treatment, the likelihood of side effects and the clinical feasibility of the presence of additional anti-allergic effects in the drug. Table 3 provides information on the criteria for the rational choice of antihistamines.
In recent years, topical antihistamines, in particular, aceclastine (allergodil), have taken a significant place in the treatment of allergic rhinitis. This drug has a quick (within 20-30 minutes) symptomatic effect, improves mucociliary clearance, has no significant systemic side effects. Its clinical efficacy in the treatment of allergic rhinitis is at least comparable to 3rd generation oral antihistamines.
The most promising oral antihistamines (the "gold" standard of therapy) are deservedly considered loratadine and cetirizine.
Loratadine (clarithin) is the most commonly prescribed “new” antihistamine that does not have a sedative effect, significant drug interactions, including interactions with alcohol, and is recommended for use by patients of all age groups. An excellent safety profile of clarithin allowed the drug to be included in the list of OTC drugs.
Cetirizine (zyrtec) is the only drug that has proven effective in treating mild bronchial asthma, which allows it to be used as a basic drug, especially in young children, when the inhaled route of prescribing is difficult. It has been shown that long-term administration of cetirizine in children with early atopic syndrome can reduce the risk of progression of atopic conditions in the future.
Literature.
Report on international consensus on the diagnosis and treatment of rhinitis. Russian rhinology. - 1996. - No. 4. - S. 2-44.
Ament P., Paterson A. Drug Interactions with the Nonsedating Antihistamines. \\\\ American Family Physician. - 1997. - v. 56. - N1.- p.223-228.
Berman S. Pediatric Decision Making. Second Edition. Philadelphia .: B.C. Decker, Inc. 1991.480 p.
Canonica W. Mechanisms of Anti-allergic Treatment. \\\\ ACI News. 1994. Supl.3.p.11-13.
Davies R. Rhinitis: Mechanisms and Management. In: Mackay I. Royal Society of Medicine Services Limited. 1989.
Peggs J., Shimp L., Opdycke R. Antihistamines: The Old and The New. \\\\ American Family Physician. - 1995. - v. 52. - N.2. - p. 593-600.
(P. Creticos, 1993).
1st generation - act on peripheral and central H 1 histamine receptors, cause a sedative effect, do not have an additional anti-allergic effect.
- bamipin ( Soventolointment)
- dimetinden ( Fenistil)
- diphenhydramine ( Dimimedrol, Benadryl)
- clemastine ( Tavegyl)
- mebhydrolin ( Diazolin, Omeril)
- oxatomide ( Tinset)
- promethazine ( Pipolphen, Diprazin)
- pheniramine ( Avil)
- chifenadine ( Phencarol)
- chloropyramine ( Suprastin)
with antiserotonin action
- dimebon ( Dimebone)
- setastin ( Loderix)
- cyproheptadine ( Peritol)
2nd generation - act on histamine receptors and stabilize the mast cell membrane.
- ketotifen ( Zaditen and etc.)
3rd generation - act only on peripheral H 1 histamine receptors, do not cause a sedative effect, stabilize the mast cell membrane and have an additional anti-allergic effect.
- acrivastin ( Semprex)
- astemizole ( Hismanal, Histalong, Astemisan, Astelong)
- terfenadine ( Trexyl, Teridin, Tofrin)
- fexofenadine ( Telfast)
- loratadine ( Claritine)
- cetirizine ( Zyrtec)
- ebastin ( Kestine)
- acelastine ( Allergodil)
- levocabastine ( Histimet)
Table 2. Characterization of modern antihistamines.
Table 3. Criteria for choosing antihistamines
1. The feasibility of choosing a drug with an additional anti-allergic effect:
- year-round allergic rhinitis;
- seasonal allergic rhinitis (conjunctivitis) with a duration of seasonal exacerbations\u003e 2 weeks;
- chronic urticaria;
- atopic dermatitis;
- allergic contact dermatitis;
- early atopic syndrome in children.
2. The patient has specific problems:
- children under 12 years old:
- loratadine ( Claritine)
- cetirizine ( Zyrtec)
- terfenadine ( Trexyl)
- astemizole ( Hismanal)
- dimetinden ( Fenistil)
- children 1-4 years old with early atopic syndrome:
- cetirizine ( Zyrtec)
- loratadine ( Claritine)
- pregnant women:
- loratadine ( Claritine)
- fexofenadine ( Telfast)
- astemizole ( Hismanal)
- women during lactation:
- clemastine ( Tavegyl)
- pheniramine ( Avil)
- patients with renal failure:
- loratadine ( Claritine)
- astemizole ( Hismanal)
- terfenadine ( Trexyl)
- patients with impaired liver function:
- loratadine ( Claritine)
- cetirizine ( Zytrec)
- fexofenadine ( Telfast)
· Antihistamines
- ... historically, the term “antihistamines” means drugs that block H1-histamine receptors, and drugs that act on H2-histamine receptors and which are used as antisecretory drugs (cimetidine, ranitidine, famotidine, etc.) are called H2 - histamine blockers.
In 1942, the first N-receptor antagonists were created that met the requirements for drugs. From this period began the era of the massive use of antihistamines in wide medical practice.
Classical N-receptor antagonists (or 1st generation drugs) represented mainly by 6 groups of chemical compounds derived from ethanolamine, phenothiazine, ethylenediamine, alkylamine, piperazine, piperidine. At the same time, up to several dozen of these drugs were present on the global pharmaceutical market.
This situation was caused by some common special properties of H-receptor antagonists of the first generation. The most important of them can be summarized as follows. These drugs in therapeutic doses relatively weakly bind H-receptors, being competitive histamine antagonists, which explains the relatively short-term effect of their action and the need to use repeated therapeutic doses during the day.
I generation drugs do not have a very high selectivity of action, and therefore, in therapeutic doses, they can block the receptors of other mediators (M-cholinergic receptors, 5HT receptors, α-adrenergic receptors, D-receptors), which is associated with a number of undesirable side effects (on the cardiovascular system, gastrointestinal tract, vision, mucous membranes, etc.). The central effects of these drugs, which cross the blood-brain barrier and have a sedative effect, as well as stimulate appetite, are well known. A very important undesirable property of first-generation drugs is tachyphylaxis, that is, a decrease in the antihistamine effect with prolonged (more than 7-10 days) use. That is why the presence of a large number of H-receptor antagonists on the pharmaceutical market was required in order to be able to replace one drug with another during prolonged treatment.
Despite the undesirable properties of the 1st generation H-receptor antagonists mentioned, these drugs are still widely used, and in some cases even for advanced medical reasons. With the accumulation of clinical and pharmacological experience, it turned out that in certain clinical situations, properties that are undesirable under ordinary conditions (sedative effect, the ability to block other types of receptors, short duration of action) can be used for therapeutic purposes, when dose fractionality can be used. The undoubted advantage of antagonists of H-receptors of the first generation is the dosage forms, including injection. In addition, one cannot but take into account the colossal medical experience, as well as the relatively low cost of these drugs in comparison with the drugs of the latest generation.
1st generation antihistamines: diphenhydramine (diphenhydramine, benadryl, allergen), clemastine (tavegil), doxylamine (decaprine, donormyl), diphenylpyraline, bromodiphenhydramine, dimenhydrinate (dedalon, dramamine), chloropyramine (suprastin), pyrilamine, antephenamine, antephenamine, antephenamine, antephenamine, antephenamine, antephenamine, antephenamine, antephenamine, antephenin pheniramine (avil), mebhydrolin (diazolin), quifenadine (fenkarol), sequifenadine (bicarfen), promethazine (fenergan, diprazine, pipolfen), trimeprazine (teralen), oxemazine, alimemazine, cyclizine, hydroxyzine (atizin) cyproheptadine (peritol).
The following pharmacological properties are most characteristic for antihistamines of the 1st generation (sedatives):
Sedative action, is determined by the fact that most antihistamines of the first generation, easily dissolving in lipids, penetrate well through the blood-brain barrier and bind to the H1 receptors of the brain. Perhaps their sedative effect consists of blocking the central serotonin and acetylcholine receptors. The degree of manifestation of the sedative effect of the first generation varies in different drugs and in different patients from moderate to severe and increases when combined with alcohol and psychotropic drugs. Some of them are used as sleeping pills (doxylamine). Rarely, instead of sedation, psychomotor agitation occurs (more often in moderate therapeutic doses in children and in high toxic doses in adults). Due to the sedative effect, most drugs cannot be used during work that requires attention. All first-generation drugs potentiate the effects of sedative and hypnotic drugs, narcotic and non-narcotic analgesics, monoamine oxidase inhibitors and alcohol.
Anxiolytic effectcharacteristic of hydroxysine may be due to the suppression of activity in certain areas of the subcortical region of the central nervous system.
Atropine-like reactionsassociated with the anticholinergic properties of the drugs are most characteristic of ethanolamines and ethylenediamines. Manifested by dry mouth and nasopharynx, urinary retention, constipation, tachycardia and visual impairment. These properties provide the effectiveness of the discussed drugs for non-allergic rhinitis. At the same time, they can increase obstruction in bronchial asthma (due to an increase in sputum viscosity), cause exacerbation of glaucoma and lead to infravesical obstruction in prostate adenoma, etc.
Anti-emetic and anti-coughing effectalso probably associated with a central anticholinergic effect of drugs. Some antihistamines (diphenhydramine, promethazine, cyclizine, meklizin) reduce the stimulation of the vestibular receptors and inhibit the function of the labyrinth, and therefore can be used for movement diseases.
A number of H1-histamine blockers reduce symptoms of parkinsonismdue to central inhibition of the effects of acetylcholine.
Antitussive effectmost characteristic of diphenhydramine, it is realized due to the direct action on the cough center in the medulla oblongata.
Antiserotonin effect, primarily characteristic of cyproheptadine, determines its use in migraine.
α1 blocking effectwith peripheral vasodilation, especially inherent in the antihistamine phenothiazine series, can lead to a transient decrease in blood pressure in sensitive individuals.
Local anesthetic (cocaine-like) actioncharacteristic of most antihistamines (occurs due to a decrease in the permeability of membranes for sodium ions). Diphenhydramine and promethazine are stronger local anesthetics than novocaine. However, they have systemic quinidine-like effects, manifested by lengthening the refractory phase and the development of ventricular tachycardia.
Tachyphylaxis: decrease in antihistamine activity with prolonged use, confirming the need for alternation of drugs every 2-3 weeks.
It should be notedthat antihistamines of the first generation differ from the second generation in the short duration of exposure with a relatively rapid onset of clinical effect. Many of them are available in parenteral forms.The strategy for creating new antihistamines changed after the heterogeneity of H receptors was established in the late 60s. It turned out that the external manifestations of allergy are mediated by the action of histamine on the 1st type of receptor. And although 4 types of these receptors have become known at present, it remains clear that the external manifestations of an allergic reaction are the result of the action of histamine on the 1st type of receptors (H1 receptors). Therefore, the task was to create highly selective H1 receptor blockers in the absence of blockade of other receptors and the loss of other undesirable properties, in particular sedation and tachyphylaxis.
In the late 70s, a compound (terfenadine) was found that accidentally met the above requirements. Subsequently, the list of compounds with such properties was replenished with new agents that made up the group of H1 receptor antagonists of the second generation, which at that time included astemizole, loratadine, cyterisin, ebastine. Terfenadine and astemizole have now left the pharmaceutical market due to a known undesirable side effect on the cardiovascular system.
All representatives of second-generation drugs belonging to different types of chemical compounds share similar properties, indicating their advantages over first-generation drugs. II generation drugs have a high affinity for H1 receptors, most of them are non-competitive blockers. the latter property requires a brief explanation. The hypothesis that the blockade is not competitive due to the selective binding of the H1 receptor seems reasonable, but not in the region of active centers responsible for binding to histamine, but in other areas. Therefore, histamine cannot displace the antagonist bound to the receptor, which is retained for a long time in a bound state, preventing the conformation of the receptor that occurs when it interacts with a mediator (histamine) and is necessary for signal transmission to the cell.
So, for drugs of the second generation is characteristic high affinity for the H1 receptor. The binding strength of the antagonist with the H1 receptor ensures the duration of its action, and therefore the possibility of a single dose of the drug during the day. Due to the high selectivity of the blockade of precisely H1 receptors, second-generation drugs in therapeutic doses do not block the receptors of other mediators and, accordingly, do not have undesirable side effects characteristic of antagonists of H1 receptors of the first generation. The physico-chemical properties of second-generation drugs can virtually eliminate or significantly reduce their penetration through the blood-brain barrier and thereby eliminate central effects, including sedation. Even for cetirizine, which in a number of studies has shown a sedative effect in a slightly larger percentage of cases than in placebo groups, this effect is incomparably less pronounced than in the precursor of cetirizine - hydroxyzine. Finally, these drugs for the most part do not show tachyphylaxis, that is, they can be used for a long time by patients without replacement with other antihistamines. Also, these drugs can be used for wider clinical indications: in chronic allergic conditions without changing one antagonist to another, in bronchial asthma, combined with manifestations requiring the appointment of H1 receptor antagonists. finally, with the creation of antagonists of H1 receptors of the second generation, the possibility has opened up of the use of antihistamines by people engaged in activities that require increased attention, which is especially important in our time.
Some of the drugs of the first generation in their individual properties are close to the drugs of the second generation. So, for example, acrivastin, the use of which involves fractional use (3 times a day), is a fairly highly selective blocker of H1 receptors, is only partially metabolized, and rarely has a sedative effect. The original class of antihistamines created by domestic researchers (M.D. Mashkovsky, M.E. Kaminka) are quinuclidine derivatives. The well-known drug of this group, fencarol (chifenadine) also resembles second-generation drugs in high affinity for H1 receptors, low sedation, and a good safety profile. In addition to the antagonistic effect on H1 receptors, it increases the activity of diaminoxidase (histaminase) and therefore has an additional anti-allergic effect due to the destruction of histamine released during an allergic reaction.
II generation antihistamines: acrivastin (semprex), astemizole (gismanal), dimetinden (fenistil), oxatomide (tinset), terfenadine (bronal, histadine), azelastine (allergodil), levocabastine (histimet), misolastine, loratadine (claritin), epine, epin bastin (kestin), bamipin (soventol).
The most common for II generation antihistamines (non-sedative) are the following properties:
High specificity and high affinity for H1 receptorsin the absence of influence on choline and serotonin receptors.
Rapid onset of clinical effect and duration of action. Prolongation can be achieved due to high protein binding, cumulation of the drug and its metabolites in the body, and delayed excretion.
Minimal sedationwhen using drugs in therapeutic doses. It is explained by the weak passage of the blood-brain barrier due to the structural features of these agents. Some especially sensitive individuals may experience moderate drowsiness, which is rarely the cause of drug discontinuation.
Lack of tachyphylaxiswith prolonged use.
The ability to block potassium channels of the heart muscle, which is associated with prolongation of the QT interval and heart rhythm disturbance. The risk of this side effect increases with the combination of antihistamines with antifungal (ketoconazole and intraconazole), macrolides (erythromycin and clarithromycin), antidepressants (fluoxetine, sertraline and paroxetine), with the use of grapefruit juice, as well as in patients with severe liver function.
Lack of parenteral formhowever, some of them (azelastine, levocabastine, bamipine) are available in the form of topical application.III generation antihistamines (metabolites). Further ways to improve the antagonists of H1 receptors were prompted, unfortunately, by negative circumstances. The fact is that most of the drugs in this series were prodrugs, that is, pharmacologically active metabolites are formed in the body from the initial form, which have a metabolic effect. If the initial compound, unlike its metabolites, gave undesirable effects, then the occurrence of conditions under which its concentration in the body increased could lead to serious consequences. This is exactly what happened at one time with the drugs terfenadine and astemizole. Of the antagonists of H1 receptors known at that time, only cetirizine was not a prodrug, but the actual medicine. It is the final pharmacologically active metabolite of the drug of the first generation of hydroxyzine. Using cetirizine as an example, it was shown that a slight metabolic modification of the original molecule allows a qualitatively new pharmacological preparation to be obtained. A similar approach was used to obtain a new antihistamine, fexofenadine, created on the basis of the final pharmacologically active metabolite of terfenadine. Thus, the fundamental difference between III generation antihistamines is that they are active metabolites of previous generation antihistamines. Their main feature is the inability to influence the QT interval. Currently, preparations of the third generation are represented by cetirizine and fexofenadine. These drugs do not pass the blood-brain barrier and therefore do not have side effects from the central nervous system. In addition, modern antihistamines have some significant additional anti-allergic effects: they reduce the expression of adhesion molecules (ICAM-1) and suppress eosinophil-induced secretion of IL-8, GM-CSF and sICAM-1 from epithelial cells, reduce the severity of allergen-induced bronchospasm, reduce the phenomenon of bronchial hyperreactivity.
III generation antihistamines: cetirizine (zirtec), fexofenadine (telfast).
Thus, antihistamines are antiallergic agents of truly untapped possibilities. Directing research efforts to increase the affinity of these compounds for H1 receptors, on the one hand, and expanding and enhancing the ability to inhibit the function of target cells, on the other hand, will allow us to productively realize the idea of \u200b\u200bantiallergic multifunctional drugs that can supplant glucocorticosteroids as drugs with a better safety profile.
Professor L.A. Goryachkina
RMAPO, Moscow
For 60 years antihistamines (AGP) used in the treatment of the following allergic diseases:
- allergic rhinitis (seasonal and year-round)
- allergic conjunctivitis
- allergic skin diseases (atopic dermatitis, acute and chronic urticaria, Quincke edema, etc.)
- allergic reactions to insect bites and stings
- prevention of complications with SIT and others.
Attempts to use the newly obtained antihistamines more widely than logically justified discredit even those drugs whose effectiveness for treating histaminergic symptoms is extremely high.
Allergic diseases, in particular, allergic rhinitis, atopic asthma, chronic idiopathic urticaria, atopic dermatitis, are among the most common pathological conditions in humans. Although these diseases usually do not pose a threat to life, nevertheless they can significantly impair the quality of life of patients. Allergic diseases have a similar pathogenesis and, in fact, can be considered as local manifestations of systemic allergic inflammation. Histamine is one of the main mediators of allergic reactions, therefore, blockers of histamine H 1 receptors remain the means of choice in the treatment of allergic diseases, especially rhinitis and chronic urticaria.